

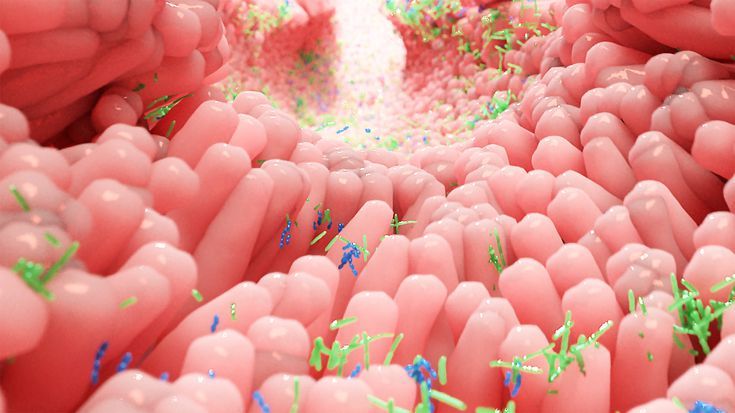
The human body is in daily contact with potentially toxic and infectious substances in the gastrointestinal tract (GIT). The GIT protects the intestinal integrity by allowing the passage of beneficial agents and blocking the path of harmful substances.
Under normal conditions, a healthy intestinal barrier (gut lining) prevents toxic elements from entering the blood stream. However, factors such as stress, an unhealthy diet, excessive alcohol, antibiotics, and drug consumption can disturb the composition of the intestinal microbiota (gut flora) and homeostasis of the intestinal barrier of the intestine, leading to increased intestinal permeability.
The Intestinal Hy-permeability can allow the entry of harmful agents through the junctions of the intestinal epithelium, to leak into the blood stream and affect various organs and systems and is known as LEAKY GUT SYNDROME (LGS)!
An increase in intestinal permeability is a sign of a disturbed intestinal barrier (2). According to the leaky gut syndrome (LGS) hypothesis, intestinal hyperpermeability may allow the entry of harmful microorganisms, toxins, or undigested food particles through the junctions of the intestinal epithelium, reaching the bloodstream and being able to affect the hormonal, immune, nervous, respiratory or reproductive systems (3).
Thus, dysfunction of the intestinal epithelial barrier and increased permeability results in a “leaky gut” that is associated with intestinal disorders such as inflammatory bowel disease (IBD), irritable bowel syndrome (IBS), alcoholic liver disease (ALD), nonalcoholic fatty liver disease (NAFLD), steatohepatitis, liver cirrhosis, and collagen diseases (1).
Leaky gut syndrome is also associated with extra-intestinal diseases (diseases that are not related to intestinal disorders) such as heart diseases, obesity, type 1 diabetes mellitus, and celiac disease (1).
Thus, the mucosal barrier is crucial to protect the body from exogenous harmful biological and chemical agents, such as microorganisms and environmental pollutants. The function of gastrointestinal epithelial barrier is to protect against the entry of foreign antigens and microorganisms, while allowing the absorption of essential nutrients, water and electrolytes (1,57).
The intestinal barrier consists of four components: microbial barrier, biochemical barrier, physical barrier and immune barrier (1,57).
The microbial barrier is the intestinal microbiota, located in the lumen of an intestine. The microbiota produces many metabolically active compounds that show antimicrobial activity and affect the function of the entire intestinal barrier. Commensal bacteria digest certain food components and also compete with pathogens for nutrients (1,57).
The biochemical barrier is mucus, which contains about 98% water (1) and, among others, mucins, glycoproteins, IgA antibodies, antimicrobial substances, produced by microorganisms—bacteria, viruses, fungi and intestinal cells. Mucus coats epithelial cells and protects them from the harmful effects of pathogenic microorganisms and toxic substances (57).
The physical (epithelial) barrier is an essential component of the entire intestinal barrier. It consists of a single layer of specialized cells: enterocytes, goblet cells (produce mucins), Paneth cells (produce antimicrobial peptides and proteins), enteroendocrine cells, M cells and intestinal stem cells. These cells undergo renewal every 3–5 days. Epithelial cells have a variety of functions and are closely interconnected (1,57).
The immune barrier is associated with the presence of lymphoid tissue in the intestines known as gut-associated lymphoid tissue (GALT). The GALT system is located in the mucosa and submucosa of the intestines, directly beneath the epithelial cells. This system consists of intraepithelial lymphocytes (IELs), Peyer’s patches, which are clustered lymphoid papules, and lymphocyte clusters. The GALT system has also been found to contain antigen-presenting cells (APCs), T lymphocytes, B lymphocytes, plasma cells, as well as macrophages, mast cells and dendritic cells (DC). The secretory IgA antibody (sIgA) is synthesized in the intestine in particular (1,57).
This picture is taken from reference 1
This picture is taken from reference 57
The intestinal barrier is a selective barrier—its function is to allow the transport of digested food essential for the body’s function, but at the same time to keep harmful substances and microorganisms in the intestinal lumen, which requires strict regulation of the barrier’s permeability (1,57). This transport is regulated by tight junctions (TJ) (1,57). The TJ between enterocytes play a key role in providing an intestinal barrier. These junctions are composed of proteins, including occludin, claudin and junctional adhesion molecules (JAMs) and peripheral proteins known as zonula occludens (ZO-1, ZO-2, ZO-3), which bind to actin filaments (1).
The primary role of zonulin is to dynamically open and close tight junctions between epithelial cells, thereby regulating paracellular permeability. When zonulin is released and its pathway is activated, it triggers intracellular signaling (including protein kinase C and cytoskeleton rearrangement) that leads to reversible disassembly of tight junction proteins such as ZO-1 and occludin. Increased zonulin production has been observed under the presence of certain bacteria and food components, such as gliadin peptides found in gluten. Excessive release of zonulin results in weakening of TJ and consequent passage of antigens into the vicinity of immune cells and into the circulatory system. As a result, local inflammation develops and activated immune cells and cytokines can affect other organs or trigger immune-related diseases, e.g., autoimmunity (58).
Elevated zonulin levels and increased permeability have been associated with several chronic inflammatory and autoimmune conditions, including celiac disease, type 1 diabetes, inflammatory bowel disease, and some neuroinflammatory and neurodegenerative disorders (59). Because of its strong association with barrier dysfunction, zonulin is being explored as a biomarker of impaired gut barrier function in various autoimmune and chronic inflammatory diseases.
Pollution and climate change, chemical compounds commonly used in industry and households, ecosystem changes, unhealthy diet, and stimulants, mainly alcohol, tobacco and e-cigarettes, may disrupt the epithelial barriers of the skin and mucosal surfaces. Air, water and food pollution, microplastic particles, nanoparticles, household chemicals and tobacco smoke are the most common epithelial barrier disrupting factors (57).
Therefore, pathogenesis of inflammatory bowel and leaky gut diseases is associated with multifactorial causes as discussed below.
Gut Microbiome and Leaky Gut

The gut has more than 100 trillion bacteria (4), with an aggregate biomass of approximately 1.5 kg (5) composed of more than 200 microbial strains in an individual and more than 90% of the dominant bacterial species belonging to the phylum Firmicutes and Bacteroidetes (6,7). The gut genome has between 20,000 and 25,000 protein-coding genes, while the genome of the bacterial community in the human intestine is approximately 9 million genes (8) capable of providing characteristics that the human genome does not possess.
The intestinal microbiota of humans is comprised of bacteria, viruses, fungi, and protozoa, although mainly bacteria. The main bacterial species that inhabit the tract are those of the phylum Bacteroidetes (Prevotella, Porphyromonas), Firmicutes (Clostridium, Eubacteria), and Actinobacteria (Bifidobacterium) (9). However, the intestinal microbiota in adults is found to have low amount of Firmicutes and an abundance of Bacteroidetes (9). Other species we can find are those of the Lactobacillus, Streptococcus, and Escherichia coli, although to a lesser extent (9). Thus, the microbial community that harbors the gastrointestinal tract is diverse and host specific.
The intestinal microflora (gut flora) is regarded as crucial for the health status of the host for maintaining homeostasis; wherein, the relationship between the host and the microbiota is mutualistic. However, a breakdown of this balance, known as dysbiosis, could contribute to the development of the disease (10).
The gut microbiota has a crucial function in the energy and metabolic regulation of the human being since it provides up to 10% of our calories consumed daily (10). Through the fermentation of food, the microbiota releases metabolites and short-chain fatty acids, which have anti-inflammatory properties and contribute to intestinal homeostasis (11).
The microbiota is considered (together with environmental, genetic, and immunological factors) (12) an essential element in the development of inflammatory bowel disease or irritable bowel syndrome, either as a mechanism that predisposes or protects against the development of intestinal inflammation (6,12).
Bottom line, the gut microbiota performs several functions, such as regulating various nutrients and regulating the immune system, which can prevent and treat intestinal inflammation (13).
Factors That Influence Intestinal Permeability
- Dysbiosis – The gut microbiota influences intestinal permeability through regulation of tight junction proteins, mucus synthesis/degradation, and immune interactions. Dysbiosis, or imbalances in gut bacteria, can increase permeability. Microbial products and inflammation can activate pro-inflammatory pathways that disrupt tight junctions, further compromising barrier function.
The composition of the microbiota changes continuously throughout life, and many factors influence its composition. Thus, it mainly varies according to factors such as diet, age, genes, drugs ingested, and environmental, physical, and psychological stress.
The imbalance in intestinal microbiota alters the tight intercellular junctions (TJ) that allow access to pathogens and toxins (bacterial lipopolysaccharides, LPS). Additionally, it induces stimulation of mucosa-associated lymphatic tissue (MALT) with the activation of the inflammatory cascade (leukocytes, cytokines, and TNF-α), the establishment of a chronic inflammation process and, consequently, massive tissue damage (14).
- Infections or Inflammation – Infections can also play a role in disrupting the intestinal barrier. Chronic inflammation from diseases such as IBD/IBS or infections caused due to food poisoning can erode the intestinal lining, increasing permeability. For example, Helicobacter pylori can infect the human stomach. This bacterium is known to increase intestinal permeability due to the redistribution of the ZO-1 protein from the TJ (15). Elevated proinflammatory markers, insulin resistance, obesity, and metabolic syndromes are associated with altered intestinal integrity. Chronic drug use (especially NSAIDs), alcohol abuse, and radiation therapy can also damage the lining.
- Antibiotics and Drugs – The gut microbiota can also be affected by antibiotics or other drugs. A study on the effects of antibiotics with different modes of action on the composition of the human microbiota showed that antibiotic treatment could increase or decrease certain species of the intestinal microbiota (16) as they destroy both beneficial and non-beneficial bacteria.
Macrolides are among the most widely used antibiotics in children and adults. It has been shown that consumption of antibiotics, for a prolonged time, in children led to an alteration in the intestinal microbiota, which decreased Actinobacteria and increased Bacteroides and Proteobacteria.
On the other hand, clarithromycin, the first antibiotic used to eradicate Helicobacter pylori, showed a decrease in actinobacteria and firmicutes, with an increase in Bacteroides and Proteobacteria after H. pylori eradication.
Some studies showed that vancomycin decreased fecal microbiota diversity due to reduced Firmicutes and increased Proteobacteria.
Ciprofloxacin was found to reduce Firmicutes and Actinobacteria (specifically Bifidobacterium) and increased Bacteroides, while clindamycin decreased Lactobacillus and Bifidobacteriaceae (17).
In addition, other drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, or paracetamol damage the gastric and intestinal mucosa and are associated with gastrointestinal complications. Patients who are long-term users of these drugs may show a decrease in absorption capacity and a possible increase in bowel permeability (18).
- Alcohol – Alcohol consumption alters the gut microbiome (gut dysbiosis), which can lower beneficial bacteria and increase pathogenic organisms, exacerbating barrier dysfunction. Intestinal barrier dysfunction or increased permeability (leaky gut) allows translocation of endotoxins (lipopolysaccharides, LPS), peptidoglycan, and other macromolecules into the circulation, which triggers systemic and hepatic inflammatory responses (1).
Additionally, Alcohol increases intestinal permeability by disrupting tight junctions between intestinal cells, damaging the barrier through metabolites like acetaldehyde, and promoting gut dysbiosis and inflammation (1).
Alcohol and its primary metabolite acetaldehyde can directly interfere with tight junction proteins (such as occludin and E-cadherin) via phosphorylation, oxidative stress, and nitrosative damage, leading to increased paracellular permeability.
High concentrations of alcohol are particularly damaging to the ileum, but even lower doses can increase permeability without causing dysbiosis (1).
- Diet – The diet strongly influences the microbial composition and functions of the gut. Diet plays a critical role in modulating intestinal permeability. Diets high in saturated fats, fructose, emulsifiers, refined carbohydrates/sugar, processed food, and alcohol can impair the intestinal barrier function and increase permeability.

The intestinal hyperpermeability cases tend to be located in countries with a Western culture, where a diet rich in fats and refined carbohydrates predominates (19). The refined carbohydrates and fats induce cellular inflammation through intestinal dysbiosis and affect both the metabolism of the gastrointestinal tract of the host and immune homeostasis (20). Additionally, food additives have been related to permeable bowel syndrome. A recent review describes the ability of additives to increase intestinal permeability by interfering with tight junctions (TJs), promoting the passage of harmful substances to the organism (21).
Also, Deficiencies in vitamin A and D, lower levels of butyrate (a short-chain fatty acid produced by gut microbiota), and changes in diet or microbiota composition negatively affect barrier integrity.
Conversely, nutrients like prebiotic fibers, probiotics, polyphenols, glutamine, methionine, vitamin D, and zinc can enhance barrier function.
- Stress – Stress profoundly affects the gut by disrupting digestion, altering the gut microbiome, increasing inflammation, and making the intestinal lining more permeable, leading to both physical and mental health consequences (1).
Main Effects of Stress on the Gut:
- Disrupted Digestion: Stress activates the “fight-or-flight” response, diverting energy away from digestion, slowing or speeding up gut motility, which can result in bloating, discomfort, diarrhea, or constipation.
- Changes in Gut Microbiome: Stress shifts the balance of gut bacteria, reducing beneficial species and promoting harmful ones—this imbalance (dysbiosis) is linked to IBS, bloating, diarrhea, and inflammation.
- Increased Gut Permeability: Stress weakens the integrity of the intestinal barrier, leading to “leaky gut,” which allows bacteria, toxins, and partially digested food to cross into the bloodstream and trigger inflammation.
- Altered Stomach Acid and Enzyme Production: Chronic stress increases stomach acid production, raising the risk for acid reflux, heartburn, or ulcers, and may also disrupt the secretion of digestive enzymes.
- Gut-Brain Feedback Loop: Gut distress can send signals back to the brain, worsening mood, anxiety, or depression, creating a vicious cycle between stress and digestive symptoms.
Symptoms of Leaky Gut

Intestinal permeability does not always present with a digestive symptom. However, some symptoms that could indicate a leaky gut are:
- Brain fog
- Headaches
- Joint pain
- Autoimmune disease
- Muscle pain
- Systemic inflammation
- Cardiovascular disease
- Metabolic syndrome
- Food sensitivity, etc.
Digestive symptoms, like bloating, diarrhea, or excessive gas, can also be early warning signs. Left untreated, these can contribute to intestinal inflammation and increased permeability.
Diseases Related to Alteration of Intestinal Permeability
Leaky gut is associated with Gastrointestinal Disorders (IBS, IBD), Extra-Intestinal Disorders (Obesity, NAFLD, Heart Failure), Autoimmune Conditions (Celiac Disease and Type 1 Diabetes) and Neurological Disorders (Depression, Dementia, Autism, Schizophrenia, and Alzheimer’s).
All of these are discussed below and shown in the picture as a schematic representation.
Intestinal Permeability and Gastro-Intestinal Disorders
- Inflammatory Bowel Disease – Inflammatory bowel disease (IBD) involves several chronic remitting diseases, of which Crohn’s disease (CD) and ulcerative colitis (UC) are probably the most common. The two differ mainly in the area of the intestine they affect: the first can appear throughout the gastrointestinal tract, although it mainly affects the ileum and cecum, and the second appears mainly in the colon and rectum (42). Although the etiology of IBD is unknown, a high level of intestinal inflammation is associated with an alteration of the tight junctions. In addition, it has been observed that patients have higher intestinal permeability than healthy subjects (54).
- Irritable Bowel Syndrome – irritable bowel syndrome (IBS) is a functional digestive disorder characterized by frequent abdominal pain related to shifts in the frequency and formation of bowel actions (43). Intestinal permeability has also been associated with the pathogenesis of IBS. Specifically, IBS patients showed lower levels of the protein zonula occludens (ZO)-1 and occludin in intestinal tissue and elevated basal levels of TNF-α, IL-1β, and IL-6 in serum (56).
Intestinal Permeability and Extra-Intestinal Disorders
- Obesity – Obesity is a chronic illness distinguished by an overabundance of adipose tissue in the body. According to the WHO (World Health Organization), obesity is defined when the BMI (Body Mass Index) is equal to or greater than 30 kg/m2 (43).

Obesity has been associated with increased intestinal permeability. In genetically obese mouse models, there is an increase in intestinal permeability and plasma endotoxins and proinflammatory cytokines, such as interleukin one beta (IL-1β), interleukin-6 (IL-6), interferon-gamma (INFγ), and tumor necrosis factor (TNF-α), compared to wild-type mice.
On the other hand, obesity induced by a high-fat diet (diet-induced obesity, DIO) is linked to changes in the population of intestinal bacteria (which is related to inflammation and increased intestinal permeability due to the reduction in gene expression linked to tight junctions (TJs) of gut lining, including ZO-1 and occluding). All this indicates that obesity-induced inflammation may be associated with changes in the integrity of the tight junctions and the intestinal microbiota (44,45).
- NAFLD and NASH – Nonalcoholic fatty liver disease (NAFLD) is a liver disease caused by excessive accumulation of fats within liver cells, not primarily caused by alcohol consumption. On the other hand, in nonalcoholic steatohepatitis (NASH), the patient, in addition to fat, can present other alterations in the liver, such as inflammation and scars (46).
Changes in the gut microbiota composition in NAFLD patients increased LPS in circulating plasma, subsequently triggering inflammation (47). These plasma LPS and proinflammatory cytokines simultaneously increase intestinal permeability (47). The increased permeability in NAFLD patients is mainly caused by ZO-1 translocation in the crypt and bacterial overgrowth in the small intestine. In general, NASH and NAFLD are highly associated with impaired tight junction (TJ) integrity (55).
- Chronic Heart Disease – Heart failure is the inability of the heart to pump enough blood to the body, so it cannot deliver the necessary oxygen and nutrients to the rest of the body. Chronic heart failure (CHF) is the most common and develops gradually over months or years (48). Patients with chronic heart failure showed a 35% increase in small bowel permeability with the lactulose/mannitol test and a 210% increase in large bowel permeability with the sucralose test.
In addition, high levels of endotoxins and inflammatory cytokines such as TNF and STNF-R1 were found. A study of the gut microbiota in such patients showed that they had massive amounts of pathogenic bacteria such as Campylobacter, Salmonella, and Candida compared to healthy subjects. All this indicates that an alteration of the barrier function in patients with CHF can induce translocations of bacteria and trigger the generation of cytokines, thus contributing to a deterioration of cardiac function (49).
Intestinal Permeability and Auto-Immune Disorders
- Celiac Disease – Celiac disease is a disease of autoimmune origin with a hereditary component caused by the ingestion of cereals that contain gluten. After the ingestion of gluten in celiac patients, gliadin, a glycoprotein present in cereals, crosses the epithelium and reaches the macrophages of the intestinal submucosa, where a response is initiated by proinflammatory molecules that recognize the protein as a cytotoxic agent and cause intestinal inflammation and increased permeability (50). This response can cause structural alterations in the TJs. It has been shown that the increase in intestinal permeability is due to an increase in the protein zonulin, which modulates tight junctions and paracellular permeability. Although gluten can trigger the release of zonulin in both healthy individuals and celiacs, the amount of zonulin produced is much higher in the latter. Celiac disease increases intestinal permeability and, consequently, induces the disruption of the integrity of the tight junctions (51).
- Type 1 Diabetes Mellitus – Diabetes mellitus is a chronic disease caused by an inability of the body to synthesize insulin or by the appearance of insulin resistance. Type 1 diabetes is characterized by an autoimmune response against the host’s pancreatic β cells, leading to insufficient insulin production (52). Certain studies indicate that there could be a relationship between intestinal barrier dysfunction and type 1 diabetes mellitus. Firstly, studies in humans with type 1 diabetes mellitus show impaired intestinal barrier function, even before the onset of the disease, and increased intestinal permeability due to the production of zonulin. On the other hand, recent studies indicate that microbial translocation contributes to the development of type 1 diabetes. Together, the results suggest an essential role of intestinal permeability in the progression of type 1 diabetes (53).
Intestinal Permeability and Neurological Disorders
Here’s where it gets really interesting – the gut and the brain are in constant conversation through nerves (vagus nerve), hormones, immune signals, and microbial metabolites — this is the gut-brain axis. When your gut is leaky, inflammatory molecules and endotoxins in your blood reach the blood-brain barrier (BBB). The BBB is supposed to be extremely selective, but under chronic inflammatory stress, its tight junctions also loosen. This “leaky brain” state allows more immune cells, inflammatory mediators, and sometimes even microbial products to enter brain tissue, triggering neuroinflammation. That can show up as brain fog, low mood, anxiety, poor memory, sleep issues, headaches, and in the long term it is being linked with conditions like depression, cognitive decline, and neurodegenerative diseases like Schizophrenia, Chronic fatigue syndrome, Autism, and Alzheimer’s disease (as shown in the picture below). In other words: a damaged gut wall can start a chain reaction that ends in a vulnerable brain!
Picture (taken from reference 1) below represents – a Relationship between leaky gut syndrome and intestinal dysbiosis with various diseases. NAFLD: nonalcoholic fatty liver disease; NASH: nonalcoholic steatohepatitis; PBC: primary biliary cholangitis; SAP: severe acute pancreatitis; DM: diabetes mellitus; SIBO: small intestinal bacterial overgrowth; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure; CD: Crohn’s disease; UC: ulcerative colitis (ulcerative colitis); IBS: inflammatory bowel diseases.
Ingredients that help Treat Leaky Gut
- Glutamine – Glutamine is considered a crucial amino acid capable of regulating the expression of tight junction proteins, allowing the membrane of intestinal cells to remain impermeable. Preclinical studies have indicated that adding glutamine improves fibrosis and intestinal inflammation (22,23).
- In T and B-lymphocytes and epithelial cells, glutamine improves anti-inflammatory IL-10 levels and decreases the production of pro-inflammatory IL-6 and IL-8 (24). Since IL-10 is vital in sustaining intestinal mucosal homeostasis, this amino acid is considered a regulator of the innate and adaptive immune response system (25).
- Glutamine with probiotics can have beneficial effects when treating intestinal permeability in patients with severe disorders. It can effectively reduce the intestinal mucosa’s permeability and the intestinal endotoxin level, restoring the mechanical damage of the intestinal barrier and thus reducing intestinal bacteria’s translocation (26).
- Polyphenols – Polyphenols have been shown to enhance tight junction integrity, increase mucus secretion, and decrease intestinal barrier permeability, thereby generally improving the intestinal defense mechanism (1). Recent studies indicate that a polyphenol-rich diet lowers the risk of intestinal barrier dysfunctions. Polyphenols such as quercetin, epigallocatechin gallate (EGCG), catechin, epicatechin, berberine, resveratrol, and curcumin have been studied intensely to provide health benefits in leaky gut-related diseases (1).
- Probiotics – In vitro studies show that various species of Lactobacillus, such as L. plantarum 299v, L. rhamnosus GG, and L. acidophilus DDS-1, may increase mucin expression and secretion by goblet cells as a mechanism to enhance barrier function and pathogen exclusion by limiting bacterial movement through of the mucosal layer (1).
- Probiotics can exhibit anti-inflammatory properties against TNF-α or IL-6. They can also strengthen the mucosal barrier and reduce intestinal permeability, upregulating TJS proteins (27).
- Another possible mechanism of action of probiotics is to produce short chain fatty acids (SCFAs) like butyrate which helps in repairing the gut lining and provide energy to colon cells (28). These factors combine to result in greater integrity of the intestine, making probiotics a fantastic therapy for reducing leaky gut (29).
- Additionally, Probiotics can increase the levels of immunoglobulin A (IgA)-producing cells in the lamina propria and promote the secretion of secretory IgA (sIgA) in the luminal layer of the mucosa. These antibodies limit epithelial colonization by binding to bacteria and their antigens, thus, contributing to intestinal homeostasis.
- Fibers and Short chain fatty acids (SCFAs) – Microbiota ferments Dietary Fibers and produces short-chain fatty acids (SCFAs) such as butyrate, propionate, and acetate. SCFAs are critical in metabolism, immunity, and intestinal barrier functions.
- For instance, butyrate provides energy for colon cells, strengthens the gut barrier to prevent “leaky gut,” and regulates the immune system by reducing inflammation (1,28,29).
- In particular, the beneficial species of Bifidobacterium bacteria and Lactobacilli are related to the production of SCFA and the immune-stimulation and inhibitory effects on the growth of harmful bacteria.
- SCFAs have a binding regulatory effect on inflammatory diseases by controlling the migration of immune cells towards the site of inflammation and modulating their activity, allowing the rapid elimination of pathogens by activating ROS as part of a defense response. The above binding process thus contributes to the reduction in damage to the host, which allows not only its survival but also the production of SCFA by intestinal bacteria (30).
- The deficiency of SCFAS and dietary fibers can compromise epithelial and mucus barrier functions by increasing gut permeability. In mice, the deficiency in consumption of dietary fibers and SCFAS production can harm intestinal barrier integrity by inhibiting Akkermansia muciniphila (1,31). A. muciniphila lives in the mucus layer of the intestine and helps maintain a strong gut lining, which is crucial for preventing inflammatory issues.
- Vitamins – In the intestinal epithelium, in vitro studies show that vitamin A and vitamin D improve the tight junctions (ZO-1, occludin, and several claudins) (1). Vitamins A and D are necessary for the integrity of the epithelium and gut microbiota and modulate immune responses at different levels. For the most part, vitamins A and D play critical functions in regulating gastrointestinal homeostasis (32). In clinical trials, these vitamins impacted the components of the mucosal barrier, including epithelial integrity, immune system, and gut microbiota.
In animal studies, these vitamins reduce microbial diversity and increase the Proteobacteria phylum (1) which are potentially pathogenic in patients with inflammatory bowel disease (IBD) (1). In human studies, vitamin A-sufficient children have more diverse microbial communities when compared to vitamin A-deficient children (35). In the intestinal epithelium, in vitro studies show that vitamin A and vitamin D improve the tight junctions (ZO-1, occludin, and several claudins) (33,34).
- Medical Herbs – Medical herbs such as – Aloe vera, ginger, DG – licorice root, marshmallow plant, hibiscus, and plantain plant – are often used to treat leaky gut-associated autoimmune disorders such as ulcerative colitis, systemic lupus erythematosus, and rheumatoid arthritis (39).
These Medical plants have phytochemicals such as organic acids, flavonoids, iridoid glycosides, saponins, chlorogenic acid, secoiridoids, berberine, sesquiterpene, and sesquiterpenoid (36). The phytochemicals have proven to treat diseases such as obesity, nonalcoholic steatohepatitis, ulcerative colitis, Crohn’s disease, food allergies, inflammatory bowel disease, and irritable bowel syndrome (37). As discussed before, a leaky gut is usually related to diseases such as dysbiosis, immune system imbalance, IBS, and nutritional deficiencies. Therefore, Herbs are useful for medical therapy and practical nutrition to help leaky gut-associated illnesses (38).
- Edible Mushrooms – Mushrooms are a great source of bioactive compounds such as ergosterol, vitamin D, phenolic compounds, terpenes, and terpenoids. In addition, mushrooms are deemed a viable source of prebiotics as they contain different polysaccharides, such as chitin, chitosan, hemicellulose, xylans, mannans, galactans, and α- and β-glucans (1).
In leaky gut-related diseases, mushrooms have been demonstrated to potentially treat pancreatitis, nonalcoholic fatty liver disease, colitis, obesity, and diabetes (1). Mushrooms were found to modulate gut microbiota by stimulating the production of catecholamines, their metabolites, and the inflammatory response.
- As mentioned, mushroom polysaccharides can also affect SCFAs production mainly butyrate, propionate, and acetate (1). Many studies have reported within the lower intestinal tract that mushroom polysaccharides contributed to the proliferation of Bacteroidetes, which is liable for most acetate and propionate production (40).
- Chaga mushrooms – Decreased the expression of tumor necrosis factor (TNF)-α, and its polysaccharide increased the proportion of Bacteroidetes and decreased that of Firmicutes at the phylum level
- Turkey tail mushrooms – Suppresses inflammatory bowel disease and its polysaccharo-peptides increase Akkermansia muciniphila population.
- Lion’s main mushrooms – It suppressed the secretion of interleukin (IL)-6, interleukin (IL)-1β, tumor necrosis factor (TNF)-α and possesses anticancer, immuno-modulating, hypolipidemic, antioxidant and neuroprotective activities.
- Improves mood and sleep disorders in patients affected by overweight or obesity.
- Possesses antihyperglycemic and antihyperlipidemic activities in diabetic rats.
- Shitake mushrooms – Its polysaccharides suppressed pro-inflammatory cytokines (tumor necrosis factor (TNF)-α, IL-6, IL-1β, and interferon (IFN)-γ) expression and colitis in mice (1).
- Possesses immunomodulation, antioxidant, and antitumor effects.
- L2 reverses the gut microbiota structure, such as the reduced Firmicutes-to-Bacteroidetes ratio (1).
- FODMAPS – FODMAP is a collective term that consists of fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (1). Nevertheless, fructose over glucose, lactose, sorbitol, mannitol, fructans (fructooligosaccharides, inulin), and galacto-oligosaccharides have shown osmotic action, increasing small bowel and lumen water content. Slow or no absorption of FODMAPs results in an increase in osmotic action, resulting in increased luminal water content and subsequent distention of the small intestine (1).
- Malabsorption or indigestion of FODMAPs results in their delivery to the large intestine, allowing exposure to the microbiota and subsequent fermentation, resulting in gas production and luminal distention of the large intestine, leading to IBS symptom induction such as gas, bloating and diarrhea (1).
- Intestinal permeability has also been associated with the pathogenesis of irritable bowel syndrome (IBS), which is treated with FODMAP. IBS patients showed lower protein zonula occludens (ZO)-1 and occludin in intestinal tissue. They showed an increase in the production of cytokines in peripheral blood mononuclear cells (PBMCs), and these patients (most notably those with diarrhea) showed basal levels of elevated serum TNF-α, IL-1β, and IL-6 (1). Therefore, low-FODMAP diet has been recommended to provide irritable bowel syndrome patients with a treatment approach that can effectively relieve most symptoms in most patients and is now supported by high-quality evidence, including randomized controlled trials (1,41).
- Physical Activity – Research results indicate that physical activity regulates the level of intestinal barrier permeability in a manner that is dependent on exercise intensity. Regular, moderate-intensity physical exercise has a positive effect on intestinal epithelial status and intestinal barrier integrity. Exercise increases the diversity of intestinal microbiome, which, as mentioned above, contributes to maintaining the integrity of the intestinal barrier, and also shows anti-inflammatory and antioxidant effects. Moderate physical activity can be an adjunctive factor in the treatment of leaky gut (57). High-intensity physical activity, typical of competitive or extreme sports, is correlated with a high incidence of gastrointestinal disorders and symptoms of increased intestinal permeability. This is a stressor for the body, causing hypoxia (lack of oxygen) and dehydration in intestinal cells due to redistribution of blood and fluids in the body (57).
TO SUM IT UP:
The intestinal microbiota is essential to maintain the intestinal epithelium’s integrity and homeostasis. A qualitative and quantitative imbalance in the composition of the intestinal microbiota or dysbiosis contributes to intestinal barrier dysfunction and leaky gut syndrome. Certain infections, an unhealthy diet, stress, excessive use of antibiotics and other drugs, and alcohol can influence increased intestinal permeability and cause leaky gut syndrome.
The intestinal hyperpermeability produced in leaky gut syndrome leads to an alteration of the tight junctions, the entry of toxic agents into the blood, and dysfunction in organs and systems. Leaky gut syndrome therapy should include diet modification avoiding fats, sugars, additives, and ultra-processed foods, and the appropriate supplementation of probiotics/prebiotics, arginine, glutamine, polyphenols, vitamins, fibers, medical herbs, edible mushrooms, and FODMAPs with regular to moderate intensity workout.
Several studies have shown that these ingredients influence the modulation of intestinal immunity, regulation of the intestinal epithelial barrier, amelioration of mucosal abnormalities, and growth of epithelial cells.
REFERENCES:
- Aleman RS, Moncada M, Aryana KJ. Leaky Gut and the Ingredients That Help Treat It: A Review. Molecules. 2023 Jan 7;28(2):619. doi: 10.3390/molecules28020619. PMID: 36677677; PMCID: PMC9862683.
- Binienda A., Twardowska A., Makaro A., Salaga M. Dietary carbohydrates and lipids in the pathogenesis of leaky gut syndrome: An overview. Int. J. Mol. Sci. 2020;21:8368. doi: 10.3390/ijms21218368.
- Obrenovich M. Leaky Gut, Leaky Brain? Microorganisms. 2018;6:107. doi: 10.3390/microorganisms6040107.
- Mileo A.M., Nistico P., Miccadei S. Polyphenols: Immunomodulatory and Therapeutic Implication in Colorectal Cancer. Front. Immunol. 2019;10:729. doi: 10.3389/fimmu.2019.00729.
- Xu J., Gordon J. Honor thy symbionts. Proc. Natl. Acad. Sci. USA. 2003;100:10452–10459. doi: 10.1073/pnas.1734063100.
- Basso P.J., Fonseca M.T., Bonfá G., Alves V.B., Sales-Campos H., Nardini V., Cardoso C.R. Association among genetic predisposition, gut microbiota, and host immune response in the etiopathogenesis of inflammatory bowel disease. Braz. J. Med. Biol. Res. 2014;47:727–737. doi: 10.1590/1414-431X20143932.
- Yu L.C.-H. Microbiota dysbiosis and barrier dysfunction in inflammatory bowel disease and colorectal cancers: Exploring a common ground hypothesis. J. Biomed. Sci. 2018;25:79. doi: 10.1186/s12929-018-0483-8.
- Yang L., Lu X., Nossa C., Francois F., Peek R., Pei Z. Inflammation and Intestinal Metaplasia of the Distal Esophagus Are Associated with Alterations in the Microbiome. Gastroenterology. 2009;137:588–597. doi: 10.1053/j.gastro.2009.04.046.
- Serra D., Almeida L.M., Dinis T.C.P. Dietary polyphenols: A novel strategy to modulate microbiota-gut-brain axis. Trends Food Sci. Technol. 2018;78:224–233. doi: 10.1016/j.tifs.2018.06.007.
- Gorkiewicz G., Moschen A. Gut microbiome: A new player in gastrointestinal disease. Virchows Arch. 2017;472:159–172. doi: 10.1007/s00428-017-2277-x.
- Yap Y., Mariño E. An Insight Into the Intestinal Web of Mucosal Immunity, Microbiota, and Diet in Inflammation. Front. Immunol. 2018;9:2617. doi: 10.3389/fimmu.2018.02617.
- Rinninella E., Raoul P., Cintoni M., Franceschi F., Miggiano G.A., Gasbarrini A., Mele M.C. What is the healthy gut microbiota composition? Microorganisms. 2019;7:14. doi: 10.3390/microorganisms7010014.
- Boulangé C.L., Neves A.L., Chilloux J., Nicholson J.K., Dumas M.-E. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Med. 2016;8:42. doi: 10.1186/s13073-016-0303-2.
- Cappello F., Rappa F., Canepa F., Carini F., Mazzola M., Tomasello G., Bonaventura G., Giuliana G., Leone A., Saguto D., et al. Probiotics can cure oral aphthous-like ulcers in inflammatory bowel disease patients. Int. J. Mol. Sci. 2019;20:5026. doi: 10.3390/ijms20205026.
- Fedwick J.P., Lapointe T.K., Meddings J.B., Sherman P.M., Buret A.G. Helicobacter pylori activates myosin light-chain kinase to disrupt claudin-4 and claudin-5. Infect. Immun. 2005;73:7844–7852. doi: 10.1128/IAI.73.12.7844-7852.2005.
- Pérez-Cobas A.E., Artacho A., Knecht H., Ferrús M.L., Friedrichs A., Ott S.J., Moya A., Latorre A., Gosalbes M.J. Differential effects of antibiotic therapy on gut microbiota. PLoS ONE. 2013;8:e80201. doi: 10.1371/journal.pone.0080201.
- Iizumi T., Battaglia T., Ruiz V., Perez Perez G.I. Gut Microbiome and Antibiotics. Arch. Med. Res. 2017;48:727–734. doi: 10.1016/j.arcmed.2017.11.004.
- Bhatt A.P., Gunasekara D.B., Speer J., Reed M.I., Peña A.N., Midkiff B.R., Magness S.T., Bultman S.J., Allbritton N.L., Redinbo M.R. NSAID-Induced Leaky Gut. ACS Infect. Dis. 2018;4:46–52. doi: 10.1021/acsinfecdis.7b00139.
- Steinert R.E., Feinle-Bisset C., Asarian L., Horowitz M., Beglinger C., Geary N. Ghrelin, CCK, GLP-1, and PYY roles. Physiol. Rev. 2017;97:411–463. doi: 10.1152/physrev.00031.2014.
- Michielan A., D’Incà R. Intestinal Permeability in IBD. Mediators Inflamm. 2015;2015:628157. doi: 10.1155/2015/628157.
- Lerner A., Matthias T. Food additives and autoimmune disease. Autoimmun. Rev. 2015;14:479–489. doi: 10.1016/j.autrev.2015.01.009.
- Kretzmann N.A., Fillmann H., Mauriz J.L., Marroni C.A., Marroni N., Gonzalez-Gallego J., Tunon M.J. Effects of glutamine in colitis. Inflamm. Bowel Dis. 2008;14:1504–1513. doi: 10.1002/ibd.20543.
- Balasubramanian K., Kumar S., Singh R.R., Sharma U., Ahuja V., Makharia G.K., Jagannathan N.R. Colonic mucosa metabolism. Magn. Reson. Imaging. 2009;27:79–86.
- Coeffier M., Marion R., Ducrotte P., Dechelotte P. Glutamine effect on cytokines. Clin. Nutr. 2003;22:407–413.
- Mantovani A., Marchesi F. IL-10 and macrophages. Immunity. 2014;40:637–639.
- Wang J., Ji H., Wang S., Liu H., Zhang W., Zhang D., Wang Y. Lactobacillus plantarum barrier function. Front. Microbiol. 2018;9:1953.
- Patel A., Lindström C., Patel A., Prajapati J.B., Holst O. Probiotic lactic acid bacteria. Int. J. Fermented Foods. 2012;1:87–101.
- Moeinian M. Butyrate and probiotics in colitis. World J. Gastroenterol. 2014;20:10876.
- Tsai Y.L., Lin T.L., Chang C.J., Wu T.R., Lai W.F., Lu C.C., Lai H.C. Probiotics and disease. J. Biomed. Sci. 2019;26:3.
- Tan J., McKenzie C., Potamitis M., Thorburn A., Mackay C., Macia L. SCFAs role. Adv. Immunol. 2014;121:91–119.
- Desai M., Seekatz A., Koropatkin N., Kamada N., Hickey C., Wolter M., Pudlo N., Kitamoto S., Terrapon N., Muller A. Fiber-deprived microbiota. Cell. 2016;167:1339–1353.
- Said H.M. Vitamin absorption. Biochem. J. 2011;437:357–372.
- Kong J., Zhang Z., Musch M.W., Ning G., Sun J., Hart J., Bissonnette M., Li Y.C. Vitamin D receptor role. Am. J. Physiol. 2008;294:G208–G216.
- Raftery T., Martineau A.R., Greiller C.L., Ghosh S., McNamara D., Bennett K., Meddings J., O’Sullivan M. Vitamin D supplementation. UEG J. 2015;3:294–302.
- Lv Z., Wang Y., Yang T., Zhan X., Li Z., Hu H., Li T., Chen J. Vitamin A deficiency. J. Clin. Biochem. Nutr. 2016;59:113–121.
- Niemeyer K., Bell I., Koithan M. Herbal medicine systems. J. Herb. Med. 2013;3:112–119.
- Park J., Choi T., Kang K., Choi S. Medicinal herbs and leaky gut. Biomolecules. 2021;11:284.
- Valussi M. Functional foods. Int. J. Food Sci. Nutr. 2011;63:82–89.
- Ozaka S., Sonoda A., Ariki S., Minata M., Kamiyama N., Hidano S., Ito K., Kudo Y. Herbal medicine and dysbiosis. PLoS ONE. 2022;17:e0269698.
- Ríos-Covián D., Ruas-Madiedo P., Margolles A., Gueimonde M., de los Reyes-Gavilán C., Salazar N. SCFAs and health. Front. Microbiol. 2016;7:185.
- Roberfroid M., Gibson G.R., Hoyles L., McCartney A.L., Rastall R. Prebiotics benefits. Br. J. Nutr. 2010;104:S1–S63.
- Baumgart D., Carding S. IBD immunobiology. Lancet. 2007;369:1627–1640.
- World Health Organization. Taking Action on Childhood Obesity. 2018.
- Lee J.Y., Wasinger V.C., Yau Y.Y., Chuang E., Yajnik V., Leong R.W.L. Barrier dysfunction in IBD. Proteomes. 2018;6:17.
- Parekh P.J., Balart L.A., Johnson D.A. Gut microbiome and disease. Clin. Transl. Gastroenterol. 2015;6:e91.
- Okumura R., Oseini A., Sanyal A. NASH therapies. Liver Int. 2017;37:97–103.
- Miele L., Valenza V., La Torre G., Montalto M., Cammarota G., Ricci R. Intestinal permeability in NAFLD. Hepatology. 2009;49:1877–1887.
- Morrissey R., Czer L., Shah P. Chronic Heart Failure. Am. J. Cardiovasc. Drugs. 2011;11:153–171.
- Pasini E., Aquilani R., Testa C., Baiardi P., Angioletti S. Gut flora in heart failure. JACC Heart Fail. 2016;4:220–227.
- Thomas E., Sapone A., Fasano A., Vogel N. Gliadin and permeability. J. Immunol. 2006;176:2512–2521.
- Fasano A. Zonulin and gut permeability. F1000Research. 2020;9:1–12.
- Kawasaki E. Type 1 Diabetes and autoimmunity. Clin. Pediatr. Endocrinol. 2014;23:99–105.
- Mu Q., Kirby J., Reilly C.M., Luo X.M. Leaky gut and autoimmune disease. Front. Immunol. 2017;8:598.
- Edelblum K.L., Turner J.R. Tight junction breakdown. Curr. Opin. Pharm. 2009;9:715–720.
- Lee B., Moon K.M., Kim C.Y. Tight junction regulation. J. Immunol. Res. 2018;2018:2645465.
- Fukui H. Barrier function and inflammation. Inflamm. Intest. Dis. 2016;1:135–145.
- Macura B, Kiecka A, Szczepanik M. Intestinal permeability disturbances. Clin Exp Med. 2024;24:232.
- Fasano A. Zonulin and tight junctions. Ann N Y Acad Sci. 2012;1258:25-33.
- Sturgeon C, Fasano A. Zonulin and barrier function. Tissue Barriers. 2016;4:e1251384.



