

This article focuses on the possible neuropsychological basis of leaky gut; leaky brain disease; and the microbiota’s contribution to inflammation, gastrointestinal, and blood-brain barrier (BBB) integrity.
As already indicated, in my other article titled as “leaky gut syndrome,” various diseases have been related to dysbiosis of the intestinal microbiota, microbial translocation, and dysfunction of the intestine’s barrier function.
Among them, we can highlight IBS, IBD, Obesity, Chronic Heart Failure, Autism, Alzheimer’s Disease, Cancer, Diabetes, and Autoimmune Diseases like Type 1 Diabetes and Celiac Disease (1).
Critical to any discussion on leaky barrier systems are pathogens, which, unlike commensals, have evolved elaborated mechanisms to target host barrier integrity and disseminate systemically to invade deeper tissues and organs. This pathogen gains entry into the blood stream by acting through type IV pili on bacterial surfaces, interacting with molecules on endothelial cells to disrupt the tight junctions and occasionally escape the mucosal barrier to enter the bloodstream and pass into the meninges of the brain and its surrounding membranes to cause disease and breach the blood–brain barrier (BBB) (1,4).
To understand a possible connection between leaky gut and possible leaky brain, let’s examine the barriers involved in physiological conditions.
Vital organs and biologic systems have developed barriers to host’s tissues from infection. The notable barriers are the blood brain barrier (BBB), gastrointestinal blood barrier (GBB), blood ocular and blood retinal barriers, blood placenta and blood testis barriers, the blood thymus barrier, and the blood–lung or airway barrier. Each of these barriers protects vulnerable and sensitive organs and systems (1).
A key component for the brain is the neurovasculature, which limits blood brain barrier (BBB) permeability and prevents transport of large molecules, many small molecules, and bacteria from entering the brain.

Inflammation disrupts BBB and appears to be central to brain and blood brain barrier (BBB) involvement (1).
Many diseases and physiological stressors that affect the Central Nervous System (CNS) also alter the functional integrity of the BBB (9,10). They affect the barrier’s ability to selectively restrict passage of substances from the blood to the brain. To add to this, hypoxia (lack of oxygen supply) and/or inflammation and inflammatory process alter the permeability properties and contribute to the pathophysiology of CNS diseases, leading to altered delivery of therapeutic agents to the brain (5).
Selective permeability is important and accomplished through tight junctions, composed of endothelial cells and smaller subunits anchored into the endothelium together with transmembrane proteins, such as junctional adhesion molecule, occludins, adherens, and claudins, for example. The junctional proteins in the brain are like those of the small intestine (1).
Tight junctions help protect the brain from toxins, chemicals, and pathogens that might be circulating in the bloodstream. Together with selective transport proteins, the barriers allow nutrients, oxygen, amino acids, some drugs, and glucose to enter the cerebrospinal fluid and prevent hydrophobic molecules from passing into the interfaces of blood–cerebrospinal fluid barriers, namely CSF and choroid plexus. At the same time, it allows the diffusion of many small polar molecules, dissolved gasses, hormones, and hydrophilic molecules (1).

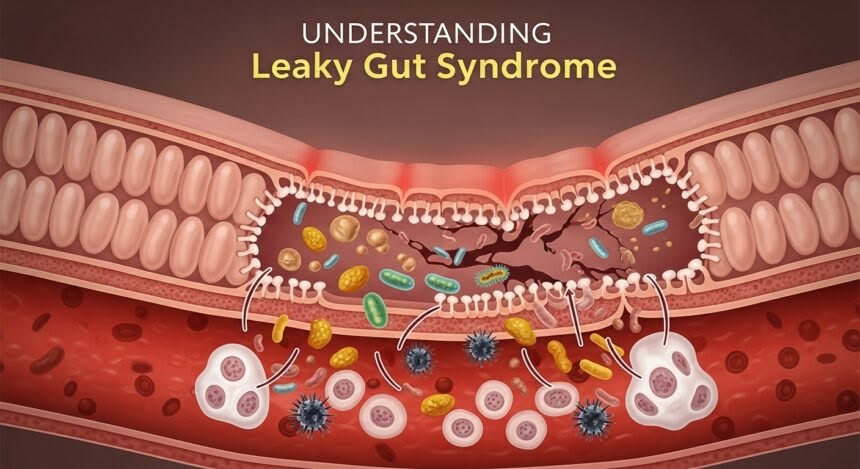
In the gut, the barrier between the body and a lumenal environment is formed by gastrointestinal mucosa, buffering nutrients, microorganisms, and toxins. The barriers are semipermeable, thus allowing efficient transport of nutrients across the epithelium, while excluding entry of potentially harmful small molecules and organisms. The exclusionary properties of the gastric and intestinal mucosa are referred to as the gastrointestinal blood barrier (GBB) (1,6).
As the barriers share common proteins and features, there is no doubt they may be susceptible to similar mechanisms of compromise or breach, either biochemically or physically. This fact underlies one basis for a plausible LEAKY GUT LEAKY BRAIN SYNDROME.
A functional blood–brain barrier is essential to maintaining central nervous system (CNS) homeostasis. BBB weakening may be a result of a disturbance in the endothelial cells due to P-glycoprotein dysfunction (7). If toxins or microorganisms breach the epithelium, they have unrestricted access to the systemic circulation. In the brain, this can occur with disruption of endothelial cells and astrocytes and involve inflammation (8).
In the gut, the alimentary canal is lined by epithelial cells that form the mucosa and, with few exceptions, the gastrointestinal epithelium is tied contiguously through tight junctions, where diversity among epithelial cells affect specific barrier functions.
When the Gut-Blood-Barrier (GBB) is breached, there are differences in localization of bacterial species. When a breach occurs, commensal bacteria deposit in the lymphatics and are not found in the blood stream, but species like Salmonella, which by definition are pathogenic – can establish infections in the blood, liver, or other organs. We have evolved with commensals and not pathogens through colonization resistance and other mechanisms, which is one reason why commensal bacteria end up in the nearby lymph nodes and are not found in distal organs despite being proximal to the epithelial linings.
Other stressors, such as glycoxidative stress (AGEs), diabetes, prolonged hyperglycemia, and obesity, are risk factors for gut–blood barrier disruption. To resolve these processes, restoration of epithelium (repair of gut lining) must happen, which can be rapid and is accomplished by a process called restitution. Advanced glycation end-products (AGEs) and crosslinking in diabetic complications and with aging may also be a mechanism for barrier protein damage with advanced age (11) and could be mediated through glycotoxins from food.
Google definition of Glycotoxins – are compounds, most commonly Advanced Glycation End-products (AGEs), that form when sugars react with proteins or fats. High levels of glycotoxins are linked to oxidative stress, inflammation, and chronic diseases like diabetes, heart disease, and Alzheimer’s.
Brain Disorders and Gut Microbiota
A dysfunction of the blood brain barrier leading to a ‘leaky brain’ can be linked to various neurological diseases, including autistic spectrum disorder (ASD) (12), dementia, Alzheimer’s disease, depression, and schizophrenia (20,13)
A breakdown in the blood brain barrier was observed in patients with major psychiatric illnesses (14) indicating that the blood–brain barrier may become ‘leaky’ in select neurological diseases that have an immunologic component, such as multiple sclerosis (MS) (15,16), Alzheimer’s disease, brain trauma, edema, brain cancers (17), amyotrophic lateral sclerosis, meningitis (4), and systemic diseases such as liver failure (18).
Moreover, co-metabolism within the gut–brain–endocrine interactome play a role in the same neurodegenerative disorders, including Parkinson’s disease (PD) and even autism, and appear to have a microbial-driven component in their pathogenesis (19).
This suggests that “microbiome of the gastrointestinal tract” play important role in controlling very integral segments of our neurobiology, mental, behavioral, and even overall health, including memory, depression, mood disruption, and anxiety (21).
Abnormal behavior and cognition impairment are found together with dysbiosis or the so-called pathobiont overgrowth syndrome, which can be one cause or consequence of leaky gut and loss of the intestinal blood barrier (21). The converse is also true – a disrupted intestinal barrier may lead to abnormal microbiome (gut dysbiosis), especially if antibiotics are involved (because antibiotics destroy both good and bad bacteria).
Antibiotic use and depression and psychiatric comorbidities occurred in irritable bowel disease and have been associated with a systemic inflammation (28). Inflammation promoting substances, like lipopolysaccharide (LPS), may pass into the blood stream and cause Inflammatory reactions that can disrupt the blood brain barrier (the so-called leaky brain) leading to increased cerebral spinal fluid (CSF) protein and their translocation.
Stress has immunologic consequences as well and plays a role in these interactions. For example, IL-1 and IL-6 (cytokines) can increase cortisol release by the stimulation of hypothalamic pituitary adrenal axis (HPA) which is in adjunct with the arm of the microbiota gut brain (MGB) axis. Stressed or Depressed patients often exhibit perturbations in this axis, resulting in elevated cortisol levels.
In addition to the microbiome, the mycobiome (fungal community) participates in modulating cytokine production, with IL-6 (22). Thus, cytokines produced at the gut reach the brain via the bloodstream, where they affect immune pathways. In the case of Autism – it was found some molecules may cross the blood–brain barrier and modulate brain area stimulation (23).
These Microbial interactions with the BBB may involve crossing of brain microvascular endothelial cells. Therefore, the microbiota gut brain (MGB) axis can indirectly affect the brain – as a function of the network of metabolic communication signaling together with – other molecules moving between the gut and the brain, between host metabolism, and pathogenic or commensal resident gastrointestinal bacterial metabolism.
Thus, the MGB axis and its metabolite cross-talk, referred to collectively as the biochemical co-metabolism that occurs between the host and the microbiota – acts to modulate both the gastrointestinal tract and the central nervous system (21,26,27). Ultimately, the intestinal microbiota can communicate with the brain via these axes to influence aspects of brain development and behavior and influence a broad spectrum of diseases (21).
These results allow us to draw a conclusion that “Blood brain barrier disruption is related to gastrointestinal barrier breach which contributes to neuroinflammation, and neuro-behavioral changes as seen in the case of “Autism (ASD), Celiac Disease and other neurological disorders” – which evidently supports the concept of Leaky Gut and Leaky Brain.
However, some studies show that probiotics could potentially help prevent leaky gut or the consequences of symptoms and possibly restore colonization resistance to the species contributing to ‘leakiness’ (24). This is because – Probiotics produce short chain fatty acids such as acetate, propionate and butyrate. Among which butyrate helps in the strengthening of the gut lining (repairs leaky gut). Similarly, propionate had shown protective effects on the BBB by inhibiting pathways associated with non-specific microbial infections via a CD14-dependent mechanism (25).
Discussed below is the example of an autoimmune condition – “Celiac Disease” – which elucidates a connection between Leaky Gut and Leaky Brain!
Leaky Gut and Celiac Disease
“Leaky gut syndrome”, is long associated with celiac disease (CD), and has attracted much attention in recent years and for decades.
Celiac disease is an autoimmune disease, characterized by inflammation of the intestinal mucosa in the small intestine due to an immune response and the loss of tolerance to dietary gluten and gliadin proteins found in wheat, barley, and rye (1,2).
Gluten and gluten sensitivity are considered to trigger this syndrome in individuals genetically predisposed to celiac disease. Tissue transglutaminase (tTG) is the main auto-antigen (Alaedini and Green, 2008), whereas gut histopathology shows variable degrees of small bowel mucosal villi atrophy (1,2).
CD affects 0.3–1.5% of the general population, approximately 1 of 120–300 people in Europe and America (Morello et al., 2003; Bingley et al., 2004).
The function of our immune system is to defend ourselves against infections and other diseases. However, in autoimmune conditions (immune response), our body becomes the aggressor and attacks the body’s own cells, causing damage (3).
How digestion-resistant Gliadin protein and peptides (A-gliadin P31–43) can induce a stress response or trigger innate immune responses may be one mechanism in the loss of tolerance to gluten (29). The innate immune response has been shown to increase zonulin, which is a modulator of intercellular tight junctions and trafficking of macromolecules important in tolerance and immune responses. Dysregulation of the zonulin pathway can increase the permeability of tight junctions and render individuals susceptible to possible autoimmune disorders, cancer, and inflammation (30).
According to the literature, the nervous system may be one of the elective sites of gluten-mediated pathogenesis, including cross-reacting antibodies, immune-complex deposition, direct neurotoxicity, other immune-mediated factors, and deficiency of vitamin and other nutrients secondary to chronic malabsorption (Zelnik et al., 2004; Bushara, 2005; Abenavoli, 2010; Parisi et al., 2015).
Medical literature suggests a potential relationship between cerebral hypoperfusion (inadequate blood flow to the brain) and intestinal hyperemia (excessive blood flow to the intestine) in the context of celiac disease from immune-mediated or endothelial damage due to immune-complex deposition likely involving antibodies against gliadin (De Santis et al., 1997).
Therefore, Celiac disease (CD) can be considered a complex multi-organ disorder with highly variable extra-intestinal complications, including neurological involvement.
Cerebellar ataxia, peripheral neuropathy, seizures, headache, cognitive impairment, and neuropsychiatric diseases are complications frequently reported (2).
These neurological manifestations may either precede or follow the disease – may be present at the onset of the typical disease or become clinically evident during its course (Hadjivassiliou et al., 2002a, 2010, 2014; Briani et al., 2008).
- Gluten ataxia or Cerebellar ataxia – “Gluten ataxia” is one of the first recognized symptoms (Cooke and Smith, 1966) and the most frequent neurological disturbance in CD (Hadjivassiliou et al., 2015). Recent studies showed deposits of antibodies against tTG on cerebellar blood vessels, adding support to a blood-brain barrier (BBB) dysfunction in CD (Hadjivassiliou et al., 2006, 2015). Interestingly, gluten ataxia is not usually related to intestinal manifestations or vitamin deficiency, and improvement with a Gluten Free Diet (GFD) is possible (Hadjivassiliou et al., 2006).
Definition from google – “Gluten ataxia” is an autoimmune neurological condition where the immune system attacks the brain’s coordination center, the cerebellum (cerebral ataxia), in response to gluten. Symptoms include poor balance and coordination, difficulty walking, speech issues, and vision problems, which worsen over time as long as gluten is consumed.
- Peripheral Neuropathy – Peripheral neuropathy is the second most common neurological manifestation of CD (up to half of patients) after cerebellar ataxia, and can appear even before diagnosis (Chin et al., 2003; Chin and Latov, 2005). A previous study on 32 consecutive adult patients complaining of peripheral neuropathy, autonomic dysfunction, or both, and showing anti-neuronal antibodies found no response despite the adoption of a GFD (Tursi et al., 2006).
Definition from google – Peripheral neuropathy is damage to the peripheral nervous system, which can cause symptoms like numbness, tingling, burning or stabbing pain, and muscle weakness, often in the hands and feet. Causes include diabetes, injuries, infections, autoimmune diseases, and certain medications.
- Epilepsy – A bidirectional link between epilepsy and CD has been established in several studies, although not all (Vieira et al., 2013), with rates of prevalence from 3.5 to 7.2% (Cooke and Smith, 1966; Zelnik et al., 2004; Bushara, 2005; Uygur-Bayramicli and Ozel, 2011; Hadjivassiliou et al., 2014; Parisi et al., 2015).
A large population-based cohort study observed an increased risk of CD in subjects of all ages, including children, even when epilepsy was independently restricted to patients receiving the diagnosis of epilepsy and those with prescriptions of antiepileptic drugs (Ludvigsson et al., 2012). The hypotheses accounting for epilepsy in CD included a gluten-mediated toxicity, an immune-induced cortical damage, the presence of cerebral calcifications, and vitamins/trace elements malabsorption.
Definition of epilepsy – Epilepsy is a brain disorder characterized by recurrent seizures, which are caused by abnormal electrical activity in the brain. Symptoms include repeated seizures that can involve loss of consciousness, twitching or jerking movements, stiffening, or unusual sensations and behaviors. Causes can range from brain damage and genetics to unknown factors, and the condition is managed with treatments like medication, though it is not contagious.
- Headaches – Celiac disease is linked to headaches particularly migraines, with a higher prevalence of headaches in people with the condition compared to the general population. Factors like gut-brain interactions, inflammation, and nutritional deficiencies are thought to contribute to headaches in those with celiac disease. For many, following a gluten-free diet can lead to fewer and less severe headaches, especially if the headache is triggered by accidental gluten ingestion (Hadjivassiliou et al., 2001).
- Cognitive Impairment and Dementia – Adult CD patients often complain of mild cognitive symptoms called “brain fog,” which improves when gluten-restriction is started, but re-appears with dietary contamination (Lichtwark et al., 2014; Yelland, 2017). Concentration and attention difficulties, episodic memory deficits, word-retrieval problems, reduced mental acuity, and episodes of confusion or disorientation are the commonly reported features (Lurie et al., 2008). In some severely affected patients, dementia can develop as acalculia (ability to perform mathematical tasks), confusion, amnesia, and personality disorders (Collin et al., 1991; Hu et al., 2006; Lurie et al., 2008; Casella et al., 2012).
- Neuropsychiatric Disorders – Several psychiatric symptoms, including depression, bipolar disorder, apathy (Carta et al., 2003, 2015; Cicarelli et al., 2003), excessive anxiety (Bushara, 2005; Campagna et al., 2017), irritability (Hernanz and Polanco, 1991), schizophrenia (De Santis et al., 1997; Bushara, 2005), eating disorders (Addolorato et al., 2001), attention-deficit/hyperactivity disorder (Karwautz et al., 2008), autism (Niederhofer and Pittschieler, 2006), and sleep complaints (Barcia et al., 2008) have been associated with CD.
Reactive anxiety that usually ameliorates with a GFD is the predominant form of anxiety disorder in these patients. Possible causative factors of mood disorders might be tryptophan deficiency secondary to chronic malabsorption (Hallert et al., 1982; Hernanz and Polanco, 1991) or co-morbidity with thyroid disease (Carta et al., 2002). Decreases in levels of serotonin, dopamine, and noradrenaline metabolites in cerebrospinal fluid (CSF) as well as tryptophan and other monoamine precursors in serum were observed in untreated patients (Hallert et al., 1982; Hernanz and Polanco, 1991). Clinical improvement was reported only after long-term administration of a GFD (>5 years) (van Hees et al., 2013), highlighting the importance of prolonged alimentary restriction on extra-intestinal CD symptoms as well.
Conclusion:
The gut certainly can influence the blood brain barrier through gastro-intestinal-derived hormonal secretion, allowing some drugs, amino acids, and small molecules to permeate barrier systems and even influence cytokine production, which is one inflammatory piece of the innate immune system issue. Bacteria can pass the human permeability and blood barriers contributing to neuroinflammation and neuro-psychiatric illnesses, thus, supporting the construct of Leaky Gut and Leaky Brain.
References:
- Obrenovich MEM. Leaky Gut, Leaky Brain? Microorganisms. 2018 Oct 18;6(4):107. doi: 10.3390/microorganisms6040107. PMID: 30340384; PMCID: PMC6313445.
- Pennisi M, Bramanti A, Cantone M, Pennisi G, Bella R, Lanza G. Neurophysiology of the “Celiac Brain”: Disentangling Gut-Brain Connections. Front Neurosci. 2017 Sep 5;11:498. doi: 10.3389/fnins.2017.00498. PMID: 28928632; PMCID: PMC5591866.
- Fasano A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol. Rev. 2011;91:151–175. doi: 10.1152/physrev.00003.2008. [DOI] [PubMed] [Google Scholar]
- 11.Kolappan S., Coureuil M., Yu X., Nassif X., Egelman E.H., Craig L. Structure of the Neisseria meningitidis type IV pilus. Nat. Commun. 2016;7:13015. doi: 10.1038/ncomms13015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lochhead J.J., Ronaldson P.T., Davis T.P. Hypoxic stress and inflammatory pain disrupt blood-brain barrier tight junctions: Implications for drug delivery to the central nervous system. AAPS J. 2017;19:910–920. doi: 10.1208/s12248-017-0076-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Braun L.D., Cornford E.M., Oldendorf W.H. Newborn rabbit blood-brain barrier is selectively permeable and differs substantially from the adult. J. Neurochem. 1980;34:147–152. doi: 10.1111/j.1471-4159.1980.tb04633.x. [DOI] [PubMed] [Google Scholar]
- 21.Schinkel A.H. P-glycoprotein, a gatekeeper in the blood-brain barrier. Adv. Drug Deliv. Rev. 1999;36:179–194. doi: 10.1016/S0169-409X(98)00085-4. [DOI] [PubMed] [Google Scholar]
- 22.Abbott N.J., Rönnbäck L., Hansson E. Astrocyte-endothelial interactions at the blood-brain barrier. Nat. Rev. Neurosci. 2006;7:41–53. doi: 10.1038/nrn1824. [DOI] [PubMed] [Google Scholar]
- 15.Maes M., Kubera M., Leunis J. The gut-brain barrier in major depression: Intestinal mucosal dysfunction with an increased translocation of LPS from gram negative enterobacteria (leaky gut) plays a role in the inflammatory pathophysiology of depression. Neuro Endocrinol. Lett. 2008;29:117–124. [PubMed] [Google Scholar]
- 16.Fiorentino M., Sapone A., Senger S., Camhi S.S., Kadzielski S.M., Buie T.M., Kelly D.L., Cascella N., Fasano A. Blood-brain barrier and intestinal epithelial barrier alterations in autism spectrum disorders. Mol. Autism. 2016;7:49. doi: 10.1186/s13229-016-0110-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sell D.R., Lane M.A., Obrenovich M.E., Mattison J.A., Handy A., Ingram D.K., Cutler R.G., Roth G.S., Monnier V.M. The effect of caloric restriction on glycation and glycoxidation in skin collagen of nonhuman primates. J. Gerontol. A Biol. Sci. Med. Sci. 2003;58:508–516. doi: 10.1093/gerona/58.6.B508. [DOI] [PubMed] [Google Scholar]
- 43.Obrenovich M.E., Shola D., Schroedel K., Agahari A., Lonsdale D. The role of trace elements, thiamine and transketolase in autism and autistic spectrum disorder. Front. Biosci. 2014 doi: 10.2741/E730. [DOI] [PubMed] [Google Scholar]
- 44.Bravo J.A., Forsythe P., Chew M.V., Escaravage E., Savignac H.M., Dinan T.G., Bienenstock J., Cryan J.F. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc. Natl. Acad. Sci. USA. 2011;108:16050–16055. doi: 10.1073/pnas.1102999108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Shalev H., Serlin Y., Friedman A. Breaching the blood-brain barrier as a gate to psychiatric disorder. Cardiovasc. Psychiatry Neurol. 2009:1–7. doi: 10.1155/2009/278531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Waubant E. Biomarkers indicative of blood-brain barrier disruption in multiple sclerosis. Dis. Markers. 2006;22:235–244. doi: 10.1155/2006/709869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ortiz G.G., Pacheco-Moisés F.P., Macías-Islas M.Á., Flores-Alvarado L.J., Mireles-Ramírez M.A., González-Renovato E.D., Hernández-Navarro V.E., Sánchez-López A.L., Alatorre-Jiménez M.A. Role of the blood-brain barrier in multiple sclerosis. Arch. Med. Res. 2014;45:687–697. doi: 10.1016/j.arcmed.2014.11.013. [DOI] [PubMed] [Google Scholar]
- 48.Schneider S.W., Ludwig T., Tatenhorst L., Braune S., Oberleithner H., Senner V., Paulus W. Glioblastoma cells release factors that disrupt blood-brain barrier features. Acta Neuropathol. 2004;107:272–276. doi: 10.1007/s00401-003-0810-2. [DOI] [PubMed] [Google Scholar]
- 49.Daneman R., Prat A. The blood-brain barrier. Cold Spring Harb. Perspect. Biol. 2015;7:a020412. doi: 10.1101/cshperspect.a020412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Banack S., Caller T., Stommel E. The cyanobacteria derived toxin beta-N-methylamino-L-alanine and amyotrophic lateral sclerosis. Toxins. 2010;2:2837–2850. doi: 10.3390/toxins2122837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Perez-Muñoz M.E., Arrieta M.-C., Ramer-Tait A.E., Walter J. A critical assessment of the “sterile womb” and “in utero colonization” hypotheses: Implications for research on the pioneer infant microbiome. Microbiome. 2017;5:48. doi: 10.1186/s40168-017-0268-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Obrenovich M., Rai H., Chittoor Mana T.S., Shola D., McCloskey B., Sass C., Levison B. Dietary co-metabolism within the microbiota-gut-brain-endocrine metabolic interactome. BAO Microbiol. 2007;2:022. [Google Scholar]
- 54.Mello A.A., Mello M.F., Carpenter L.L., Price L.H. Update on stress and depression: The role of the hypothalamic-pituitary-adrenal (HPA) axis. Rev. Bras. Psiquiatr. 2003;25:231–238. doi: 10.1590/S1516-44462003000400010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Haddad-Tóvolli R., Dragano N.R.V., Ramalho A.F.S., Velloso L.A. Development and function of the blood-brain barrier in the context of metabolic control. Front. Neurosci. 2017;11:224. doi: 10.3389/fnins.2017.00224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ait-Belgnaoui A., Durand H., Cartier C., Chaumaz G., Eutamene H., Ferrier L., Houdeau J., Bueno L., Theodorou V. Prevention of gut leakiness by a probiotic treatment leads to attenuated HPA response to an acute psychological stress in rats. Psychoneuroendocrinology. 2012;37:1885–1895. doi: 10.1016/j.psyneuen.2012.03.024. [DOI] [PubMed] [Google Scholar]
- 62.Hoyles L., Snelling T., Umlai U.-K., Nicholson J.K., Carding S.R., Glen R.C., McArthur S. Microbiome–host systems interactions: Protective effects of propionate upon the blood-brain barrier. Microbiome. 2018;6:55. doi: 10.1186/s40168-018-0439-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Main B.S., Minter M.R. Microbial immuno-communication in neurodegenerative diseases. Front. Neurosci. 2017;11:151. doi: 10.3389/fnins.2017.00151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lochhead J.J., Ronaldson P.T., Davis T.P. Hypoxic stress and inflammatory pain disrupt blood-brain barrier tight junctions: Implications for drug delivery to the central nervous system. AAPS J. 2017;19:910–920. doi: 10.1208/s12248-017-0076-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Maes M., Kubera M., Leunis J. The gut-brain barrier in major depression: Intestinal mucosal dysfunction with an increased translocation of LPS from gram negative enterobacteria (leaky gut) plays a role in the inflammatory pathophysiology of depression. Neuro Endocrinol. Lett. 2008;29:117–124. [PubMed] [Google Scholar]
- Chin R. L., Latov N. (2005). Peripheral neuropathy and Celiac disease. Curr. Treat. Options Neurol. 7, 43–48. 10.1007/s11940-005-0005-3 [DOI] [PubMed] [Google Scholar]
- Chin R. L., Sander H. W., Brannagan T. H., Green P. H., Hays A. P., Alaedini A., et al. (2003). Celiac neuropathy. Neurology 60, 1581–1585. 10.1212/01.WNL.0000063307.84039.C7 [DOI] [PubMed] [Google Scholar]



