
- pylori enters the body through the mouth, moves through the digestive system, and infects the stomach or the first part of the small intestine. The spiral-shaped bacterium uses its tail-like flagella to move around and burrow into the stomach lining. This damages the gut lining and causes inflammation.
- pyloriis a nasty pathogen that can persist in the stomach of infected persons for a lifetime, if left untreated. It provokes a chronic gastric inflammatory response, resulting in the development of several gastric pathological conditions including superficial gastritis, chronic atrophic gastritis, peptic ulcers, gastric cancer, and mucosa-associated lymphoid tissue (MALT) lymphoma (44). Although the majority of individuals colonized by H pyloriare asymptomatic, a proportion of patients develop peptic ulcers (duodenal and gastric), and an even smaller proportion develop gastric cancer. Globally, H pylori is the major cause of gastric cancer and has been classified as a Class I carcinogen by the WHO. Epidemiological studies have revealed that people with lower vegetable and micronutrient intake may be at increased risk of H. pylori infection (44).
To successfully colonize the host and establish infection, H. pylori must be able to withstand an acidic stomach and adhere to host cells. In order, to survive the harsh acidic environment of the stomach, it produces a substance called Urease, a cytoplasmic enzyme. This substance helps them neutralize the stomach acid and is largely responsible for H. pylori’s acid tolerance (1).
During active H. Pylori infection, this gram-negative bacteria uses urease to hydrolyze (convert) urea into ammonia and carbonic acid/carbon dioxide in the stomach. The ammonia byproduct buffers gastric acid leading to an increase in stomach pH to protect the organism and allow further proliferation (1). Over time, atrophy of the gastric mucosa (thinning, shrinking or wearing of gut lining) occurs permitting further multiplication of the bacteria. The preferred treatment of H. pylori infection includes a course of proton pump inhibitor (PPI) therapy (which further raises gastric pH) (5) and antibiotic agents which are also known to cause dysbiosis (because they wipe out good and bad bacteria both) and consequent gastrointestinal symptoms (6,7).
Both mucosal atrophy and gastric pH alterations have been proposed to predispose patients to SIBO (1).
In the general population, gastric secretions are strongly acidic with a pH range of 1 to 2. In non-H. pylori infection individuals, daily administration of 20 mg omeprazole (PPI) has been shown to increase gastric pH by 2 to a pH range of 3 to 4 (1).
During H. pylori infection, individuals receiving this same dose of omeprazole showed increased stomach pH by a total of 4 to a pH range of 5 to 6 (8). Within the pH range of 5 to 6, enteric bacterial load can increase by as much as 1000-fold (11). This causes abnormalities in the intestinal flora. H. pylori often infects the stomach at a young age and significantly reduces the post-infection Firmicutes to Bacteroidetes ratio at the phylum level (9). Successful eradication of H. pylori increases the amount of Bifidobacterium in the intestinal flora (10).
These bacteria (H. Pylori) are predominantly gram-negative anaerobes that produce gas with the fermentation of carbohydrates (when you eat food as in carbs). This gas fermentation allows for the detection of H. pylori infection by the urea breath test and the detection of SIBO by the hydrogen breath test (1). With that said, both bacterial load and the gas they produce contribute to the nonspecific constellation of gastrointestinal complaints (such as bloating, indigestion and acidity) as described in SIBO and H. pylori infection.
A meta-analysis study conducted by Liao L et al. (2) pooled the results of eight eligible observational studies and found that H. Pylori infection may be related to SIBO in adults. Hence, the detection of SIBO should be considered for patients with digestive symptoms and HP infection.
The study (2) results suggest that HP infection is associated with a higher prevalence of SIBO in younger adults (mean age <48 years) as compared to older adults (mean age >48 years). Subgroup analyses further indicated that the association was not significantly affected by the country of study, comorbidities, exposure to proton pump inhibitors, or methods of evaluating HP infection and SIBO (2).
Helicobacter pylori infection is also a risk factor for various gastric diseases, such as chronic gastritis, peptic ulcers (gastric and duodenal), atrophic gastritis, and gastric cancer (12,13). Increasing studies suggest that besides gastric diseases, H. Pylori infection may also be involved in the pathogenesis of some intestinal disorders (14). For example, H. Pylori infection has been linked to the risk of colorectal adenomas (15) and colorectal cancer (16), as well as functional disorders such as IBS (17), suggesting a close relationship between H. Pylori infection and disturbed intestinal homeostasis. According to research studies, impaired gastric motility and/or acidity will likely boost bacterial growth in the small intestine and increase colonization (9,10) thus, creating an environment ripe for SIBO.
Numerous studies have suggested an association of SIBO with, altered anatomy, hypochlorhydria (low stomach acid), dysmotility, immune deficiencies, and small intestinal disease and PPI use (18,19). Physically, the small intestine has relatively low-level colonized bacteria compared to the colon (8). Recent evidence from preclinical and clinical studies suggests that excessive bacterial growth in the small intestine, which is called small intestinal bacterial overgrowth (SIBO) (20), may be an underlying cause for various unspecific gastrointestinal (GI) symptoms; and the mechanisms of pathogenesis of various digestive and other systematic diseases (5). Indeed, accumulating evidence suggests that SIBO is not only observed in patients with irritable bowel syndrome (IBS) (6), but also in functional dyspepsia (7), inflammatory bowel disease (6), chronic pancreatitis (21), and liver cirrhosis (22), as well as in those with non-alcoholic fatty liver disease (NAFLD) (23), diabetes (24), systemic sclerosis (25), and Parkinson’s disease (26) etc. Therefore, these observations suggest that SIBO may be an essential pathophysiological process involved in the pathogenesis and progression of intestinal and extraintestinal disorders (27,28) and can thus, have overlapping symptoms with H. pylori.
Furthermore, PPIs are one of the most prescribed medications for the treatment of several gastrointestinal symptoms.
As stated above, several studies have shown a correlation betwwen PPI use and SIBO (8,29,30). One meta-analysis of 19 eligible studies from 1994-2016 included 7055 subjects and found a 3-fold increased risk of SIBO in patients who had received PPI therapy (29).
Also, PPI therapy is often prescribed for patients complaining of dyspepsia, a common complaint known to affect up to 21% of the world’s population (31). H. pylori infection is also more common in patients with dyspepsia (5,31). Dyspepsia is often treated with over-the-counter medications, empiric PPI therapy or sometimes antibiotic therapy (32). Antibiotic therapy again is known to disrupt the natural microbiome and predispose patients to dysbiosis (6) and potentially SIBO.
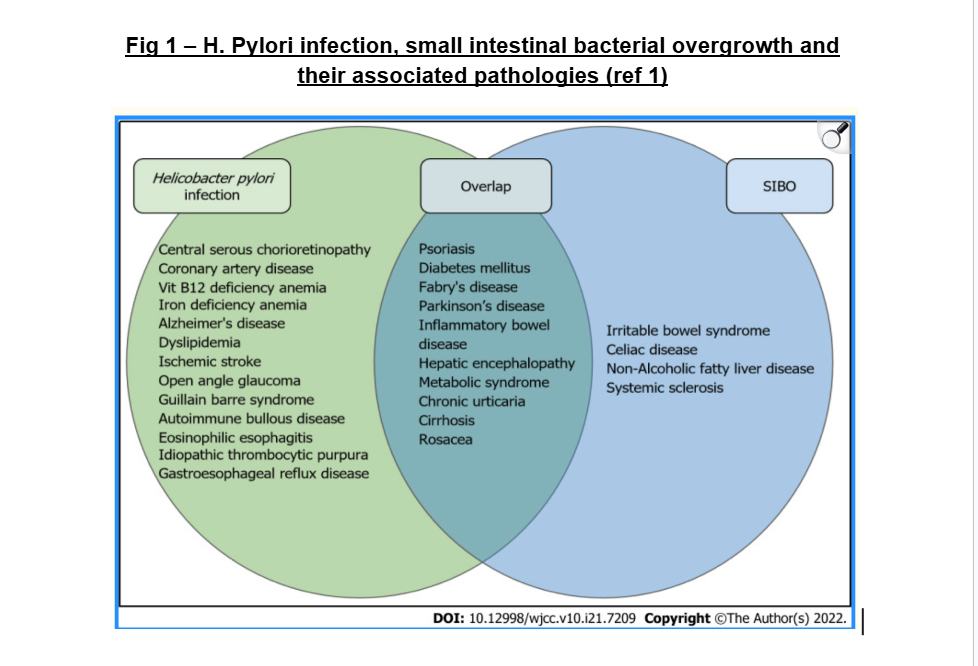
However, Independent reviews of H. pylori infection and SIBO show overlapping higher incidence (Fig 1) in patients with diabetes mellitus, metabolic syndrome, hepatic encephalopathy, chronic urticaria, psoriasis and rosacea when compared to the general population (33-36). In patients with cirrhosis and hepatic encephalopathy, the eradication of SIBO appears to improve encephalopathic symptoms; however, the treatment of H. pylori infection does not (37). Inversely, the treatment of H. pylori infection has been documented to improve chronic spontaneous urticaria (33) and rosacea (34) but the treatment of SIBO has not (See figure 1 below).
Clinical Presentation of H. Pylori and SIBO
The symptoms of SIBO and H. pylori infection are largely due to malabsorption of nutrients, inflammation and immune activation because of a high bacterial load and its byproducts. Although no single symptom is attributed to all cases of bacterial overgrowth, dyspepsia appears to be the most commonly reported in both SIBO (39) and H. pylori infection (5). In up to two-thirds of patients with SIBO, symptoms include flatulence, bloating, abdominal cramping and diarrhea. Some studies have also reported nausea and constipation (38). H. pylori infection is also frequently reported with flatulence, bloating, abdominal cramping and nausea (5). This significant symptom overlap between reported symptoms of SIBO and H. pylori infection might, in some patients, be due to the coexistence of both conditions.
Common signs and symptoms of H. Pylori infection:
- Burning sensation or pain in stomach that happens 2 to 3 hours after eating
- The pain comes and goes for several weeks and days
- The pain happens in the middle of the night when your stomach is empty
- The pain goes away when you take antiacids that reduce your stomach acid level
- Nausea or vomiting
- Indigestion
- Frequent burping or bloating
- Early fullness or satiety
- Unexplained weight loss
- Loss of appetite
Causes of H. Pylori infection (4):
- Person to Person contact – H. Pylori is contagious. The spread of H. pylori can occur directly from one person to another person or indirectly from an infected person to the environment. This is because H. pylori are found in saliva, poop and plaque on teeth. Infection can also spread by transferring the bacteria from the hands of those who haven’t thoroughly washed them after pooping, or by sharing food, water bottles and utensils with others.
- Contaminated food and water – Consuming food that was washed, prepared, or handled under unsanitary conditions, or drinking untreated water can also lead to the infection of H. Pylori.
- Unsanitary conditions – In developing countries, a combination of untreated water, crowded conditions, and poor hygiene contributes to higher H. pylori prevalence. Most people become infected as children, and parents and siblings seem to play a primary role in transmission.
Diagnostic Tests for H. Pylori infection (3):
- Urease Breath Test (UBT) – The urea breath test (UBT) is an effective method to detect H. pylori and is based on the ability of urease enzymes to convert a patient-ingested isotope-labeled urea solution into carbon dioxide and ammonia. Diagnostic accuracy of the UBT is high in people who do not have a history of gastrectomy and who have not recently taken antibiotics or PPIs. As a result, it is recommended that PPI be ceased two weeks prior and antibiotics discontinued four weeks prior to UBT analysis.
- Stool Antigen Test (SAT) – The stool antigen test (SAT) is also highly sensitive and specific, and applicable to all ages.
- Blood or Serum Test – A serological test can detect H. pylori-specific antibodies in serum, saliva, and urine. It is inexpensive, noninvasive, and convenient to detect IgG antibodies using laboratory-based serology.
- Upper Endoscopy with Biopsy – The endoscopic examination is a common method used for detecting H. pylori infections. It can detect many abnormalities, such as duodenal ulcers, gastric ulcers, and gastric antral nodules. A gastric biopsy obtained under endoscopy can be used to confirm H. pylori infection by performing invasive tests.
- Rapid Urease Test (RUT) – The Rapid Urease Test is a simple and cheap method for diagnosing H. pylori infection. Antrum mucosa and gastric body biopsies can be done simultaneously to improve the performance of H. pylori detection. PPI has a transient negative effect on the viability, morphology, and urease test of H. pylori. Thus, it is not recommended to exclusively use the RUT to diagnose H. pylori if a patient has taken a PPI in the past (Yakoob et al., 2005). Despite having many influencing factors, because RUT has a high specificity, it remains the first test choice for diagnosing H. pylori.
- PCR test – The Polymerase Chain Reaction (PCR) can detect H. pylori DNA in saliva, stool, gastric juice, and other samples, as well as virulence factor genes. It is less affected by factors, such as preservation and transportation of biopsy tissues, than in other invasive tests. Real-time PCR with different PCR kits showed excellent sensitivity and specificity in detecting H. pylori in gastric biopsies (Bénéjat et al., 2018).
Foods you should avoid if you have an H. pylori infection:
- Spicy foods – Chili peppers, mustard and anything with a strong kick can aggravate inflammation.
- Acidic foods – Citrus fruits like lemons, oranges and grapefruits might increase stomach acid and discomfort.
- Fatty foods – Fatty meats, fried foods and processed cheeses slow down digestion and keep food in your stomach longer, potentially worsening symptoms.
- Caffeinated drinks – Coffee, black tea and sodas can stimulate stomach acid production.
- Alcohol – Alcohol irritates the stomach lining and can hinder healing.
- Processed foods – These are often loaded with preservatives and additives that may irritate your stomach.
It’s important to note that everyone reacts differently. If you have specific foods that trigger heartburn or indigestion, avoid those, as well.
Foods that support the inhibition of H. Pylori
Human studies have shown that Plants and spices are not effective as single agents in eradication of H. pylori infections, but they may synergize with conventional pharmacological therapies for improved efficacy when used in combination.
- Herbs and Spices – Rachel Et al. demonstrated that several plant extracts are effective against H pylori and are obtained simply by boiling the plants. As per the study findings, among the plants that killed H pylori, turmeric was the most efficient, followed by cumin, ginger, and chilli. Other plants, such as borage, black caraway, oregano, parsley, and liquorice were also found to have bactericidal effects (41). Additionally, the anti-cancer and anti-ulcerogenic effects of ginger, cumin, liquorice, parsley, turmeric, and borage combined with their bactericidal and anti-adhesive properties, as shown in the study (41), suggests that ingestion of these six plants could have important therapeutic implications for patients with H pylori-induced peptic ulcer disease or gastric cancer. As turmeric killed 100% of organisms within 15 min, it could therefore be a useful anti-Helicobacter agent in vivo, because, if given orally, it would be able to kill H. pylori despite the short amount of time that it would remain in the stomach during digestion (41).
- Vitamin C and E – Vit (C and E) were found to be effective when used in combination with standard triple therapies for H. pylori (44). Vitamin C at high doses has been shown to inhibit the colonization of H. pylori in the stomach of Mongolian gerbils (45). Wang et al. reported the in vitro inhibition of H. pylori growth and in vivo decrease in colonization levels and inflammation scores in mice treated with vitamin C and astaxanthin (46). Treatment with astaxanthin may alters immune response to H. pylori by shifting Th1 response towards Th2 cell-response (47). Additionally, vitamin C, is known to highly concentrate in gastric mucosa and gastric juice, which may influence the course of H. pylori infections for it positively regulates the stimulation and activity of granulocytes, macrophages, and lymphocytes, and the production of immunoglobulin (44). Also, DNA damaging free radicals are usual products of chronic H. pylori infections, and supplementation with antioxidants such as vitamins (C and E) and carotenoid (astaxanthin) may be a useful strategy in combating H. pylori pathogenesis, with fruits and vegetables being the main dietary sources of these antioxidants (44).
- Broccoli sprouts – Sulforaphane (SFN), a phytochemical found in abundance in broccoli sprouts, potently induces a variety of antioxidant enzymes, and thereby protects cells from injury induced by various kinds of oxidative stresses. The data from the H. pylori infection study (42) clearly demonstrated that SFN inhibited H. pylori viability both in vitro and in vivo, and mitigated H. pylori-induced gastritis in mice and humans. Hence, the data strongly suggests that SFN contributes to the protection of GI mucosa against oxidative injury induced by H. pylori (42).
- Raw Manuka Honey – Honey is widely known for its antibacterial properties. Roland et al. demonstrated that manuka honey exhibited inhibitory activity against H. pylori isolates at 75% v/v. Findings suggest that honey may contain compounds with therapeutic potential against the isolates of H. pylori. They also demonstrated that their locally produced honey had a very good antibacterial activity comparable to the commercial honeys. (43)
Treatment and Management of H. Pylori
It includes a PPI and Antibiotics (3):
- PPIs or Proton Pump Inhibitors are a class of medications that significantly reduce the amount of acid that your stomach produces.
Drugs commonly prescribed as PPIs include:
- Omeprazole (Prilosec)
- lansoprazole
- pantoprazole
- rabeprazole
- and esomeprazole (Nexium)
The commonly used antibiotics include:
- Amoxicillin
- Clarithromycin
- Levofloxacin
- Metronidazole
- and others like Tetracycline
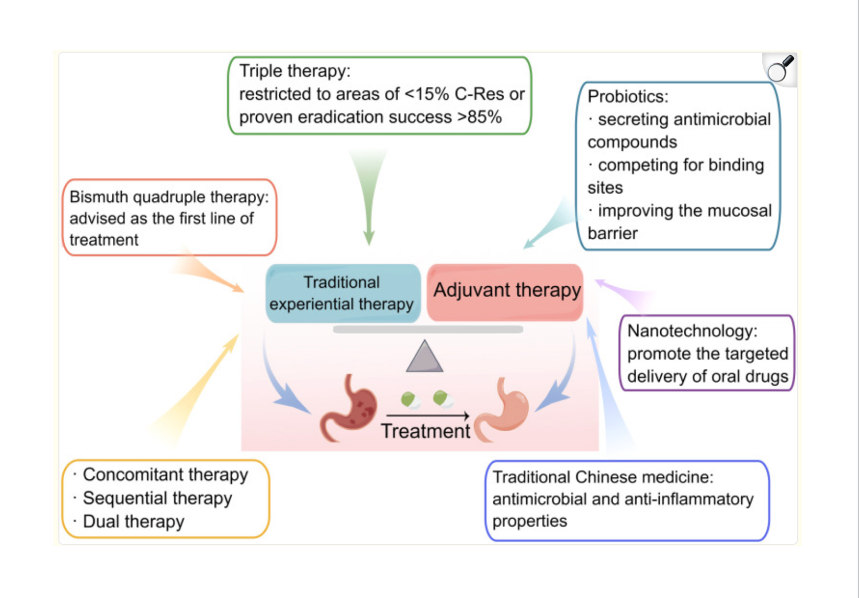
- Triple therapy – Standard triple therapy is one of the most common therapeutic methods used for H. pylori eradication, which consists of a PPI and two antibiotics. In areas where clarithromycin resistance is low, the ACG 2017 preferred treatment regimen is triple therapy with PPI, clarithromycin and amoxicillin or metronidazole. Typically, the regimen of standard triple therapy should be continued for 10–14 days until H. pylori is completely eradicated.
- Bismuth Quadruple Therapy – In locations where clarithromycin resistance is high (>20%), bismuth quadruple treatment is advised as the first-line therapy for H. pylori treatment (Malfertheiner et al., 2022). Bismuth-based quadruple therapy for 10–14 days also appears to be the most effective first-line option for penicillin-allergic patients. Usually, the PPI, bismuth, and two antibiotics make up bismuth quadruple treatment. Therefore, it includes Bismuth subsalicylate (e.g., Pepto-Bismol), tetracycline, PPI and metronidazole (5).
- Adjuvant Therapy – Involves Probiotics, Nanotechnology and Traditional Chinese Medicine (TCM)
- Probiotics – especially Lactobacillus and Limosillactobacillus reuteri, can combat H. pylori by secreting antimicrobial compounds, compete for binding sites, improve the function of the mucosal barrier, and boost the eradication effect (Ji and Yang, 2020). They can also control gut microbes to lessen negative effects and increase patient compliance. Bismuth and probiotics are an ideal combination for treating H. pylori infections.
- Nanotechnology – Oral medicine is commonly used to treat H. pylori, but some antibiotics are degraded by the gastric environment, decreasing their effectiveness. For example, amoxicillin is degraded under the acidic pH of the gastric cavity (Hassan et al., 2019). In such cases, Nanotechnology has been developed to protect and promote the targeted delivery of oral drugs. The identification of amoxicillin, when encapsulated in lipid nanoparticles, has demonstrated the potential to enhance drug retention at the infection site and shield it from adverse conditions within the stomach lumen (Lopes-de-Campos et al., 2019). Liposomes linolenic acid, a novel nanomedicine, can disrupt outer membrane barriers (aka biofilm), lead to bacterial leakage (get bacteria out of the biofilm), and deliver the drug to the proper location, which is a safe treatment method for H. pylori eradication (Zhang et al., 2020).
3. Traditional Chinese Medicine – As TCM has been widely used in treating H. pylori-related gastrointestinal diseases, Chinese herbal formulae have apparently shown advantages in treating H. pylori infection. A study has shown that berberine, an active TCM ingredient, suppresses H. pylori infection, controls mucosal inflammation, and promotes ulcer healing (Liu et al., 2022). Additionally, it has been reported that monomeric compounds derived from TCM (coptisine, evodiamine, and patchouli alcohol) have antimicrobial and anti-inflammatory properties against H. pylori. The main mechanisms of action of TCM include suppressing the replication and transcription of H. pylori, reducing urease expression, destroying the bacterial structure, downregulating the expression of virulence factors, and inhibiting the activation of signaling proteins (Li et al., 2018; Xu et al., 2021; Yang et al., 2021).
Fig 2 – Treatment of Helicobacter pylori infections (Ref 3)
Conclusion
Based on the current literature review, SIBO appears to have an increased prevalence in patients with H. pylori infection compared to the general population.
Several extra gastrointestinal conditions appear to be associated with both SIBO and H. pylori infection. And the dysbiosis created due to the attempted treatment for H. pylori infection may be related to microbial imbalance, pushing your body into a constant of low-grade inflammatory response (aka – microbiome-mediated pro-inflammatory state).
It is therefore important to recognize the signs and symptoms of H. pylori infection and treat the infection as well as the associated dysbiosis bearing in mind that persistence of gastrointestinal symptoms despite eradication of H. pylori infection could suggest coexisting SIBO.
In such cases combination of amoxicillin with rifaximin may be a useful method of treating patients with small intestinal bacterial overgrowth and concomitant H. pylori infection.
A study by Paulina Conrad et al. (40) demonstrated that the combination of amoxicillin with rifaximin may be effective already in the first-line treatment of H. pylori infection. However, the eradication rate was not satisfactory (64.0%) and may require prolongation of the therapy up to 14 days. The study also suggests that such combination treatment is justified in the case of H. pylori infection and small intestinal bacterial overgrowth as good clinical outcomes and regression of gastrointestinal symptoms are in favor of this.
References
- Dharan M, Wozny D. Helicobacter pylori infection and small intestinal bacterial overgrowth-more than what meets the eye. World J Clin Cases. 2022 Jul 26;10(21):7209-7214. doi: 10.12998/wjcc.v10.i21.7209. PMID: 36158005; PMCID: PMC9353905.
- Liao L, Su BB, Xu SP. Helicobacter pylori infection and small intestinal bacterial overgrowth: a systematic review and meta-analysis. BMC Microbiol. 2023 Dec 6;23(1):386. doi: 10.1186/s12866-023-03063-w. PMID: 38053022; PMCID: PMC10698970.
- Sun Q, Yuan C, Zhou S, Lu J, Zeng M, Cai X, Song H. Helicobacter pylori infection: a dynamic process from diagnosis to treatment. Front Cell Infect Microbiol. 2023 Oct 19;13:1257817. doi: 10.3389/fcimb.2023.1257817. PMID: 37928189; PMCID: PMC10621068.
- Kayali S, Manfredi M, Gaiani F, Bianchi L, Bizzarri B, Leandro G, Di Mario F, De’ Angelis GL. Helicobacter pylori, transmission routes and recurrence of infection: state of the art. Acta Biomed. 2018 Dec 17;89(8-S):72-76. doi: 10.23750/abm.v89i8-S.7947. PMID: 30561421; PMCID: PMC6502203.
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112:212–239. doi: 10.1038/ajg.2016.563. [DOI] [PubMed] [Google Scholar]
- McDonnell L, Gilkes A, Ashworth M, Rowland V, Harries TH, Armstrong D, White P. Association between antibiotics and gut microbiome dysbiosis in children: systematic review and meta-analysis. Gut Microbes. 2021;13:1–18. doi: 10.1080/19490976.2020.1870402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angelucci F, Cechova K, Amlerova J, Hort J. Antibiotics, gut microbiota, and Alzheimer’s disease. J Neuroinflammation. 2019;16:108. doi: 10.1186/s12974-019-1494-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Husebye E. The pathogenesis of gastrointestinal bacterial overgrowth. Chemotherapy. 2005;51 Suppl 1:1–22. doi: 10.1159/000081988. [DOI] [PubMed] [Google Scholar]
- Yang L, Zhang J, Xu J, Wei X, Yang J, Liu Y, Li H, Zhao C, Wang Y, Zhang L, Gai Z. Helicobacter pylori Infection Aggravates Dysbiosis of Gut Microbiome in Children With Gastritis. Front Cell Infect Microbiol. 2019;9:375. doi: 10.3389/fcimb.2019.00375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo Y, Zhang Y, Gerhard M, Gao JJ, Mejias-Luque R, Zhang L, Vieth M, Ma JL, Bajbouj M, Suchanek S, Liu WD, Ulm K, Quante M, Li ZX, Zhou T, Schmid R, Classen M, Li WQ, You WC, Pan KF. Effect of Helicobacter pylori on gastrointestinal microbiota: a population-based study in Linqu, a high-risk area of gastric cancer. Gut. 2020;69:1598–1607. doi: 10.1136/gutjnl-2019-319696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enko D, Kriegshäuser G. Functional 13C-urea and glucose hydrogen/methane breath tests reveal significant association of small intestinal bacterial overgrowth in individuals with active Helicobacter pylori infection. Clin Biochem. 2017;50:46–49. doi: 10.1016/j.clinbiochem.2016.08.017. [DOI] [PubMed] [Google Scholar]
- de Brito BB, da Silva FAF, Soares AS, Pereira VA, Santos MLC, Sampaio MM, et al. Pathogenesis and clinical management of Helicobacter pylori gastric Infection. World J Gastroenterol. 2019;25:5578–89.doi:10.3748/wjg.v25.i37.5578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salvatori S, Marafini I, Laudisi F, Monteleone G, Stolfi C. Helicobacter pylori and gastric Cancer: pathogenetic mechanisms. Int J Mol Sci. 2023;24. [DOI] [PMC free article] [PubMed]
- Fujimori S. Progress in elucidating the relationship between Helicobacter pylori Infection and intestinal Diseases. World J Gastroenterol. 2021;27:8040–6. doi: 10.3748/wjg.v27.i47.8040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu D, Wang M, Ke X, Wang Q, Wang J, Li D. Association between H. Pylori Infection and colorectal polyps: a Meta-analysis of Observational studies. Front Med (Lausanne) 2021;8:706036. doi: 10.3389/fmed.2021.706036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuo Y, Jing Z, Bie M, Xu C, Hao X, Wang B. Association between Helicobacter pylori Infection and the risk of Colorectal cancer: a systematic review and meta-analysis. Med (Baltim) 2020;99:e21832. doi: 10.1097/MD.0000000000021832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang C, Yin Y, Wang L, Guo X, Liu L, Qi X. Association between Helicobacter pylori Infection and irritable bowel syndrome: a systematic review and meta-analysis. Postgrad Med J. 2021. [DOI] [PubMed]
- Grace E, Shaw C, Whelan K, Andreyev HJ. Review article: small intestinal bacterial overgrowth–prevalence, clinical features, current and developing diagnostic tests, and treatment. Aliment Pharmacol Ther. 2013;38:674–688. doi: 10.1111/apt.12456. [DOI] [PubMed] [Google Scholar]
- Quigley EMM. The Spectrum of Small Intestinal Bacterial Overgrowth (SIBO) Curr Gastroenterol Rep. 2019;21:3. doi: 10.1007/s11894-019-0671-z. [DOI] [PubMed] [Google Scholar]
- Bushyhead D, Quigley EM. Small intestinal bacterial overgrowth. Gastroenterol Clin North Am. 2021;50:463–74. doi: 10.1016/j.gtc.2021.02.008. [DOI] [PubMed] [Google Scholar]
- El Kurdi B, Babar S, El Iskandarani M, Bataineh A, Lerch MM, Young M, et al. Factors that affect prevalence of small intestinal bacterial overgrowth in chronic Pancreatitis: a systematic review, Meta-analysis, and Meta-Regression. Clin Transl Gastroenterol. 2019;10:e00072. doi: 10.14309/ctg.0000000000000072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maslennikov R, Pavlov C, Ivashkin V. Small intestinal bacterial overgrowth in Cirrhosis: systematic review and meta-analysis. Hepatol Int. 2018;12:567–76. doi: 10.1007/s12072-018-9898-2. [DOI] [PubMed] [Google Scholar]
- Gudan A, Jamiol-Milc D, Hawrylkowicz V, Skonieczna-Zydecka K, Stachowska E. The prevalence of small intestinal bacterial overgrowth in patients with non-alcoholic Liver Diseases: NAFLD, NASH, Fibrosis, Cirrhosis-A systematic review, Meta-analysis and Meta-regression. Nutrients. 2022;14. [DOI] [PMC free article] [PubMed]
- Feng X, Li XQ. The prevalence of small intestinal bacterial overgrowth in Diabetes Mellitus: a systematic review and meta-analysis. Aging. 2022;14:975–88. doi: 10.18632/aging.203854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feng X, Li XQ, Jiang Z. Prevalence and predictors of small intestinal bacterial overgrowth in systemic sclerosis: a systematic review and meta-analysis. Clin Rheumatol. 2021;40:3039–51. doi: 10.1007/s10067-020-05549-8. [DOI] [PubMed] [Google Scholar]
- Li X, Feng X, Jiang Z. Association of small intestinal bacterial overgrowth with Parkinson’s Disease: a systematic review and meta-analysis. Gut Pathog. 2021;13:25. doi: 10.1186/s13099-021-00420-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel SM, Young MC. The identification and management of small intestinal bacterial overgrowth: a Functional Medicine Approach. Phys Med Rehabil Clin N Am. 2022;33:587–603. doi: 10.1016/j.pmr.2022.04.003. [DOI] [PubMed] [Google Scholar]
- Skrzydlo-Radomanska B, Cukrowska B. How to recognize and treat small intestinal bacterial overgrowth? J Clin Med. 2022;11. [DOI] [PMC free article] [PubMed]
- Su T, Lai S, Lee A, He X, Chen S. Meta-analysis: proton pump inhibitors moderately increase the risk of small intestinal bacterial overgrowth. J Gastroenterol. 2018;53:27–36. doi: 10.1007/s00535-017-1371-9. [DOI] [PubMed] [Google Scholar]
- Compare D, Pica L, Rocco A, De Giorgi F, Cuomo R, Sarnelli G, Romano M, Nardone G. Effects of long-term PPI treatment on producing bowel symptoms and SIBO. Eur J Clin Invest. 2011;41:380–386. doi: 10.1111/j.1365-2362.2010.02419.x. [DOI] [PubMed] [Google Scholar]
- Du LJ, Chen BR, Kim JJ, Kim S, Shen JH, Dai N. Helicobacter pylori eradication therapy for functional dyspepsia: Systematic review and meta-analysis. World J Gastroenterol. 2016;22:3486–3495. doi: 10.3748/wjg.v22.i12.3486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiba N, Van Zanten SJ, Sinclair P, Ferguson RA, Escobedo S, Grace E. Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment-Helicobacter pylori positive (CADET-Hp) randomised controlled trial. BMJ. 2002;324:1012–1016. doi: 10.1136/bmj.324.7344.1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campanati A, Gesuita R, Giannoni M, Piraccini F, Sandroni L, Martina E, Conocchiari L, Bendia E, Di Sario A, Offidani A. Role of small intestinal bacterial overgrowth and Helicobacter pylori infection in chronic spontaneous urticaria: a prospective analysis. Acta Derm Venereol. 2013;93:161–164. doi: 10.2340/00015555-1373. [DOI] [PubMed] [Google Scholar]
- Gravina A, Federico A, Ruocco E, Lo Schiavo A, Masarone M, Tuccillo C, Peccerillo F, Miranda A, Romano L, de Sio C, de Sio I, Persico M, Ruocco V, Riegler G, Loguercio C, Romano M. Helicobacter pylori infection but not small intestinal bacterial overgrowth may play a pathogenic role in rosacea. United European Gastroenterol J. 2015;3:17–24. doi: 10.1177/2050640614559262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gravina AG, Priadko K, Ciamarra P, Granata L, Facchiano A, Miranda A, Dallio M, Federico A, Romano M. Extra-Gastric Manifestations of Helicobacter pylori Infection. J Clin Med. 2020;9 doi: 10.3390/jcm9123887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Losurdo G, Salvatore D’Abramo F, Indellicati G, Lillo C, Ierardi E, Di Leo A. The Influence of Small Intestinal Bacterial Overgrowth in Digestive and Extra-Intestinal Disorders. Int J Mol Sci. 2020;21 doi: 10.3390/ijms21103531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abid S, Kamran M, Abid A, Butt N, Awan S, Abbas Z. Minimal Hepatic Encephalopathy: Effect of H. pylori infection and small intestinal bacterial overgrowth treatment on clinical outcomes. Sci Rep. 2020;10:10079. doi: 10.1038/s41598-020-67171-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020;115:165–178. doi:10.14309/ajg.0000000000000501. [DOI] [PubMed] [Google Scholar]
- Chojnacki C, Konrad P, Błońska A, Chojnacki J, Mędrek-Socha M. Usefulness of the hydrogen breath test in patients with functional dyspepsia. Prz Gastroenterol. 2020;15:338–342. doi: 10.5114/pg.2020.92690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Konrad P, Chojnacki J, Gąsiorowska A, Rudnicki C, Kaczka A, Chojnacki C. Therapeutic efficacy of amoxicillin and rifaximin in patients with small intestinal bacterial overgrowth and Helicobacter pylori infection. Prz Gastroenterol. 2018;13(3):213-217. doi: 10.5114/pg.2018.74228. Epub 2018 Mar 12. PMID: 30302165; PMCID: PMC6173078.
- O’Mahony R, Al-Khtheeri H, Weerasekera D, Fernando N, Vaira D, Holton J, Basset C. Bactericidal and anti-adhesive properties of culinary and medicinal plants against Helicobacter pylori. World J Gastroenterol. 2005 Dec 21;11(47):7499-507. doi: 10.3748/wjg.v11.i47.7499. PMID: 16437723; PMCID: PMC4725184.
- Yanaka A. Role of Sulforaphane in Protection of Gastrointestinal Tract Against H. pylori and NSAID-Induced Oxidative Stress. Curr Pharm Des. 2017;23(27):4066-4075. doi: 10.2174/1381612823666170207103943. PMID: 28176666; PMCID: PMC5759180.
- Ndip RN, Malange Takang AE, Echakachi CM, Malongue A, Akoachere JF, Ndip LM, Luma HN. In-vitro antimicrobial activity of selected honeys on clinical isolates of Helicobacter pylori. Afr Health Sci. 2007 Dec;7(4):228-32. PMID: 21499488; PMCID: PMC3074369.
- Ullah H, Di Minno A, Santarcangelo C, Khan H, Xiao J, Arciola CR, Daglia M. Vegetable Extracts and Nutrients Useful in the Recovery from Helicobacter pylori Infection: A Systematic Review on Clinical Trials. Molecules. 2021 Apr 14;26(8):2272. doi: 10.3390/molecules26082272. PMID: 33919894; PMCID: PMC8070974.
- Zhang H.M., Wakisaka N., Maeda O., Yamamoto T. Vitamin C Inhibits the Growth of a Bacterial Risk Factor for Gastric Carcinoma: Helicobacter Pylori. Cancer. 1997;80:1897–1903. doi: 10.1002/(SICI)1097-0142(19971115)80:10<1897::AID-CNCR4>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- Wang X., Willen R., Wadstrom T. Astaxanthin-Rich Algal Meal and Vitamin C Inhibit Helicobacter Pylori Infection in BALB/cA Mice. Antimicrob. Agents Chemother. 2000;44:2452–2457. doi: 10.1128/AAC.44.9.2452-2457.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennedsen M., Wang X., Willén R., Wadström T., Andersen L.P. Treatment of H. Pylori Infected Mice with Antioxidant Astaxanthin Reduces Gastric Inflammation, Bacterial Load and Modulates Cytokine Release by Splenocytes. Immunol. Lett. 2000;70:185–189. doi: 10.1016/S0165-2478(99)00145-5. [DOI] [PubMed] [Google Scholar]



