



6. Gastrointestinal disorders – Overgrowth of Candida in the gut has been linked with gastrointestinal diseases including Irritable bowel disease (IBD), Crohn’s disease, ulcerative colitis, gastric ulcers and duodenal ulcers. It can also cause symptoms like bloating, diarrhea, abdominal pain, cramps, and nausea (26).
Further, results from animal models argue that Candida colonization delays healing of inflammatory lesions and that inflammation promotes colonization (26). These effects may create a vicious cycle in which low-level inflammation promotes fungal colonization and fungal colonization promotes further inflammation. HOW?
Both inflammatory bowel disease (IBD) and gastrointestinal Candida colonization is associated with elevated levels of the pro-inflammatory cytokine IL-17. Therefore, effects on IL-17 levels may underlie the ability of Candida colonization to enhance inflammation (26). Also, an antibiotic treatment often leads to GI tract inflammation, which may perturb the resident bacterial community, allowing C. albicans to colonize. Furthermore, in the GI tract, C. albicans encounters and responds to varying features of the physical environment such as pH, oxygen levels and nutrient levels (47). C. albicans also responds to secretions produced in the GI tract such as bile (48). These findings argue that C. albicans is well adapted for growth in the GI tract.
Because Candida is a frequent colonizer, these effects have the potential to impact many people by exacerbating inflammation and creating a vicious cycle of colonization and inflammation – ranging from gut issues to whole body issues.
In simple words – The presence of inflammation alters bacterial colonization and the activities of the host, creating conditions that favor both high level Candida colonization and exacerbation of disease like IBD.
7. Candida and Gluten Intolerance –
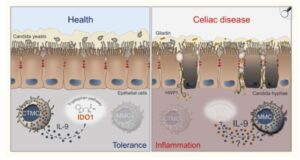
The protein HWP1 (Hyphal wall protein 1) found on the surface of Candida Albicans closely resembles gluten proteins (alpha-gliadin and gamma-gliadin). When Candida overgrows and attaches to the gut-wall using HWP1 protein, the immune system attacks this protein, but because of its similarity to gliadin (gluten protein), may also develop reactivity to gluten, leading to gluten intolerance or even autoimmune reactions such as celiac-like conditions. This phenomenon is known as molecular mimicry (49).
Furthermore, Candida overgrowth has been proposed as a cause for leaky gut, where toxins and undigested foods leak into the blood stream, leading to allergic reactions and inflammation. This makes the digestive tract more reactive to gluten and other proteins. As a result of this cross reactivity, candida may trigger gluten sensitivities by confusing the immune system, especially when gut health is compromised by candida overgrowth (50). Conversely, those with celiac disease or gluten sensitivity may be more prone to candida overgrowth because compromised gut health (due to antibiotics overuse, diabetes, pH shift, nutrient deficiencies, stress, etc) increases susceptibility to fungal imbalance as shown in the picture below (49,50).
In such cases, addressing candida overgrowth can sometimes alleviate gluten sensitivities, especially in non-celiac cases, by reducing gut inflammation and improving immune regulation. Also, for those experiencing persistent digestive symptoms, fatigue, or skin problems, considering both candida and gluten intolerance is important for accurate diagnosis and effective treatment (50).
Schematic depiction of the interactions between Candida, MCs and IL-9 in celiac disease (Ref 50).
8.Candida and Iron Deficiency – candida may make someone iron deficient by competing for iron, impairing iron absorption, and triggering host responses that further lower available iron stores.
Candida overgrowth related iron loss is particularly important to consider in individuals with chronic gut symptoms, unexplained anemia, or recurrent candida infections. Iron deficiency may manifest as fatigue, weakness, pale skin, and other symptoms.
Yes, candida overgrowth can contribute to iron deficiency through multiple mechanisms:
- Hepcidin release – The presence of candida stimulates the liver to produce antimicrobial peptide hormone called – Hepcidin – a hormone that blocks the release of iron from intestinal cells and storage tissues. Hepcidin reduces the release of iron from liver stores and decreases iron absorption from the gut to limit iron availability to pathogens. This action decreases circulating and stored iron, lowering ferritin levels (52).
- Intestinal disruption – Overgrowth of Candida can damage the gut lining, impairing iron absorption from digested food which is essential for maintaining ferritin stores. This damage decreases how much iron enters the bloodstream and can lower iron storage over time; especially if the gut microbiota is also imbalanced (51,52).
- Alteration of Microbiome – Antibiotics or other disturbances enable candida overgrowth, further disturbing iron homeostasis by impacting microbiota that might otherwise help in processing and absorption of iron (51,52).
- Nutrient Immunity – Iron homeostasis and bioavailability to either the host or invading pathogens is tightly regulated through coordination of hepcidin, iron binding proteins and several enzymes involved in iron metabolism (51,53,54). The process of sequestering iron by the host and restricting its bioavailability to invading pathogens is called nutritional immunity. During infection, immune cells surround candida as in systemic infections, sequestering iron to make it less accessible to the pathogen, which also reduces its availability for human physiological needs (51).
- Siderophore production – Candida has strong affinity for iron and produces specialized iron-binding proteins called siderophores, which scavenge iron from the host, making less iron available for absorption in the gastrointestinal tract (52).
- Multisource Uptake – It possesses multiple high-affinity iron uptake systems that allow extraction of iron from transferrin, hemoglobin, ferritin, and siderophores produced by other microbes within the host (51,52).
- Cycle of iron deficiency and candida – Low ferritin and iron deficiency can impair immune function, making it easier for candida to overgrow. Meanwhile, the overgrowth perpetuates ferritin depletion by consuming iron and triggering hepcidin production, creating a self-reinforcing cycle. Managing ferritin deficiency in candida overgrowth requires not only iron supplementation when needed but also addressing the underlying fungal imbalance to break this cycle (51).
9.Candida and Gut pH levels – Candida albicans can grow in acidic or alkaline environments, but its biology and pathogenicity shift depending on the gut’s pH. In an acidic environment, candida mainly exists as a relatively harmless yeast form. However, when the environment becomes more alkaline or neutral, candida can switch to its pathogenic fungal (hyphal) form, which is associated with overgrowth and disease symptoms in the host.
Alkaline or neutral environments – A study
(55) reports that C. albicans can actively alter the pH of its environment and induce it’s switch to the hyphal form, which is more aggressive and can invade tissue. The change in pH is caused by the release of ammonia from the cells produced during the breakdown of amino acids. This phenomenon is unprecedented in a human pathogen and may substantially impact host physiology by linking morphogenesis (candida’s switch from harmless to pathogenic form), pH adaptation, carbon metabolism, and interactions with host cells, all of which are critical for the ability of C. albicans to cause disease (55).
One environmental factor to which microorganisms must respond is extracellular pH. In the human body, pH can vary widely, from highly acidic (pH ~2) in the stomach to mildly acidic (skin and vagina), to neutral (bloodstream and parts of the gut), and even alkaline (some parts of the gut). Candida albicans, thrives in most of these sites and is highly tolerant to a wide range of environmental pH conditions, from pHs of <2 to pHs of >10 (55). albicanshas a remarkable ability to alter extracellular pH, creating a neutral environment from either acidic or alkaline starting conditions, with changes in pH from 4 to >7 in less than 12 h (55). The rise in pH induces hyphal morphogenesis, a key virulence trait of candida species, and is correlated with release of volatile ammonia from the cells.
Thus, C. albicans effectively auto induces morphogenesis under these conditions. The rise in pH is associated with the release of ammonia, a highly basic compound, as has been observed in other fungi (55).
Regarding the oral cavity, the constant mechanical action of saliva creates a true challenge for oral pathogens as it hinders their adhesion to oral tissues (56). It seems likely that, similar to other pathogenic fungi (Göttlich et al., 1995), C. albicans lipases can increase cell adhesion capacity, probably by enhancing the hydrophobicity of Candida cells following the lipase‐dependent release of fatty acids. This scenario appears to take place in patients with diabetes mellitus, whose reduced salivary flow, lower pH, and elevated levels of glucose make the oral cavity the perfect microenvironment to allow the transition from commensal to pathogenic yeast (56).
In summary, Candida’s growth, form, and immune interactions are tightly linked to the pH of its environment (57). Acidic pH tends to keep candida less virulent and more exposed to immune clearance, while alkaline pH encourages its more harmful fungal form and overgrowth.
It is important to note that stomach should be highly acidic with pH between 1 to 3 and intestinal tract should be slightly acidic (with a pH of 4 to 6.5) to avoid alkaline environment that allows candida to flourish. Additionally, a healthy vagina is naturally acidic, with a pH of 4.5 or lower, which is hostile to candida growth.
Restorative strategies for increasing the acidity of stomach:
- Consume Apple Cider Vinegar (ACV): The acid and enzymes in ACV can help kill excess yeast and support a healthy intestinal pH.
- Eat Probiotic Foods: Fermented foods like plain yogurt, kimchi, sauerkraut, and Kefir contain beneficial bacteria like Lactobacillus acidophilus that produce lactic acid and acetic acid, which help restore the correct level of acidity in the gut. Probiotic supplements can also be used.
- Cut out sugar: Candida thrives on sugar, so reducing your intake of refined carbohydrates, sugary fruits, and alcohol is critical to starving the yeast.
- Incorporate gut-friendly foods: A healthy diet that includes non-starchy vegetables, lean proteins, and healthy fats is essential for a balanced gut microbiome.
- Garlic supplements: Garlic has antimicrobial properties and may help reduce harmful bacteria that can disrupt vaginal pH balance.
- Maintain proper oral and vaginal hygiene: Avoid mouthwash, if you wear dentures clean them properly on daily basis. To maintain vaginal hygiene, avoid douching, avoid scented feminine products, and harsh soaps, as these can disrupt the vaginal microbiome and pH balance. Wearing breathable cotton underwear is also recommended.
What Functional Tests help in diagnosing Candida?
Testing is essential to differentiate the root cause of symptoms and ensure appropriate effective treatment. Following are the primary functional tests helpful in identifying candida overgrowth:
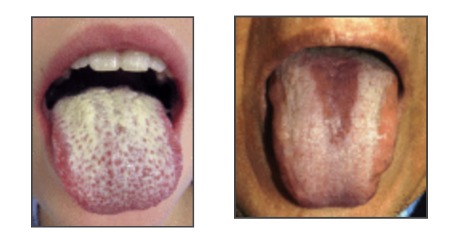
- Culture and Microscopy – Superficial candidiasis (mouth, vaginal, esophageal) is diagnosed by microscopic examination and culture of a sample from the affected area.
- Gut Microbiome test – also known as GI MAP test – involves stool analysis that helps in identifying the levels of candida present and the type of candida species present in the GI tract.
- Antigen or antibody test – This is a Blood test that measures the levels of antibodies (IgG, IgA, IgM) against Candida Albicans in the blood. Elevated levels may indicate a current or past infection.
- Urine Organic Acid test (OATS) – analyzes a urine sample to check for the presence of fungal metabolites
- Blood tests and PCR – Invasive candidiasis is diagnosed with blood cultures or PCR-based methods (e.g., T2Candida panel, which can identify candida rapidly and with high sensitivity in blood). This is the most definitive test for diagnosing a systemic (bloodstream) infection.
Treatment and Management
Candida treatment and management involve a combination of lifestyle and dietary adjustments along with some natural remedies. The specific approach depends on the type, severity, and location of the Candida infection.
Here are few steps to follow:
- Candida detox through anti-candida diet and adjusting lifestyle measures
- Herbal Antifungals
- Probiotics push back
- Pharmaceutical antifungal drugs
How to do Candida Detox?
- Avoid foods that feed unhealthy candida levels in your body – Refined sugar, refined carbohydrates, Trans fat or seed oils, dairy products, excessive amounts of animal protein, excess caffeine and alcohol, gluten (wheat, barley, rye), GMO Corn and Soy, and artificial sweeteners, sugary beverages and condiments that contain hidden sugar.
- Incorporate these foods that keep Candida at bay – Eat organic food only, eat low to moderate sugar food in moderation (berries, pineapple, apple, papaya, orange, kiwi, cherries, grapes etc), eat plenty of colorful vegetables, 2 to 4 ounces per serving of organic grass-fed animal protein, gluten free whole grains (millets, Quinoa, Oats, Buckwheat, Amaranth), add healthy fats (Olive oil, Flax oil, Hemp oil, Coconut oil, Ghee, fish oil, avocados), eat nuts and seeds in moderation, eat beans and legumes no more than 2 times per week, drink plenty of water, and incorporate herbs and spices mentioned in the table below.
- Eat fermented foods like sauerkraut, kimchi, kanji, kefir made of coconut or goat’s milk. You can also take a good quality probiotic. Probiotics contain beneficial bacteria that keep candida in check.
- Sweeteners that are safe to consume on Anti-Candida diet – Stevia, Monk Fruit, Xylitol (excess of it can cause laxative effects) and Erythritol. Erythritol is the preferred one.
- Additional Supplements support – Digestive enzymes, Betaine HCL plus pepsin, digestive bitters, OX Bile, serrapeptase as a biofilm disruptor and a good quality plant-based Multivitamin.
- Cleanse your Lymphatic system and skin – through lymphatic massage, brisk walking or swimming, deep breathing exercises, jumping on a trampoline, dry brushing, hot and cold shower, or going for saunas that involves sweating through pores of skin
- Detox your liver and support gallbladder – do this by drinking herbal teas like milk thistle, Ginger Tulsi tea, lemon water, dandelion tea, burdock root tea.
- Cleanse your kidneys and bloodstream – sip hibiscus tea for kidneys and/or, red clover tea for cleansing blood.
- Keep your bowels moving – must have at least one bowel movement per day. If you are constipated, remedies for constipation are – Triphala, senna leaves, oxy powder, magnesium citrate or enema.
- Stimulate your Vagus Nerve – by singing your favorite song, chanting a mantra like OM, gargling with warm water early morning, yoga, meditation and deep belly breathing exercises, splashing cold water on face, or taking cold shower.